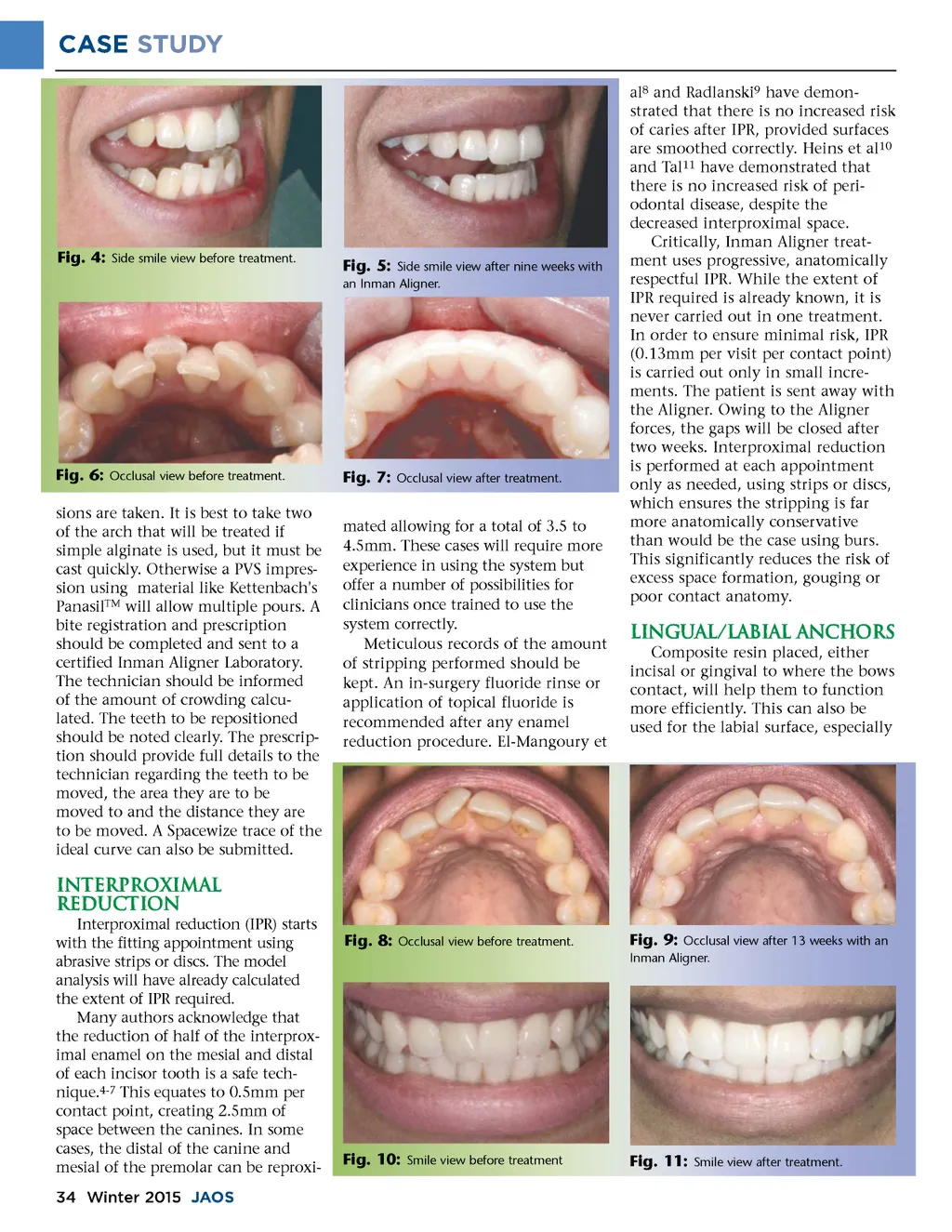
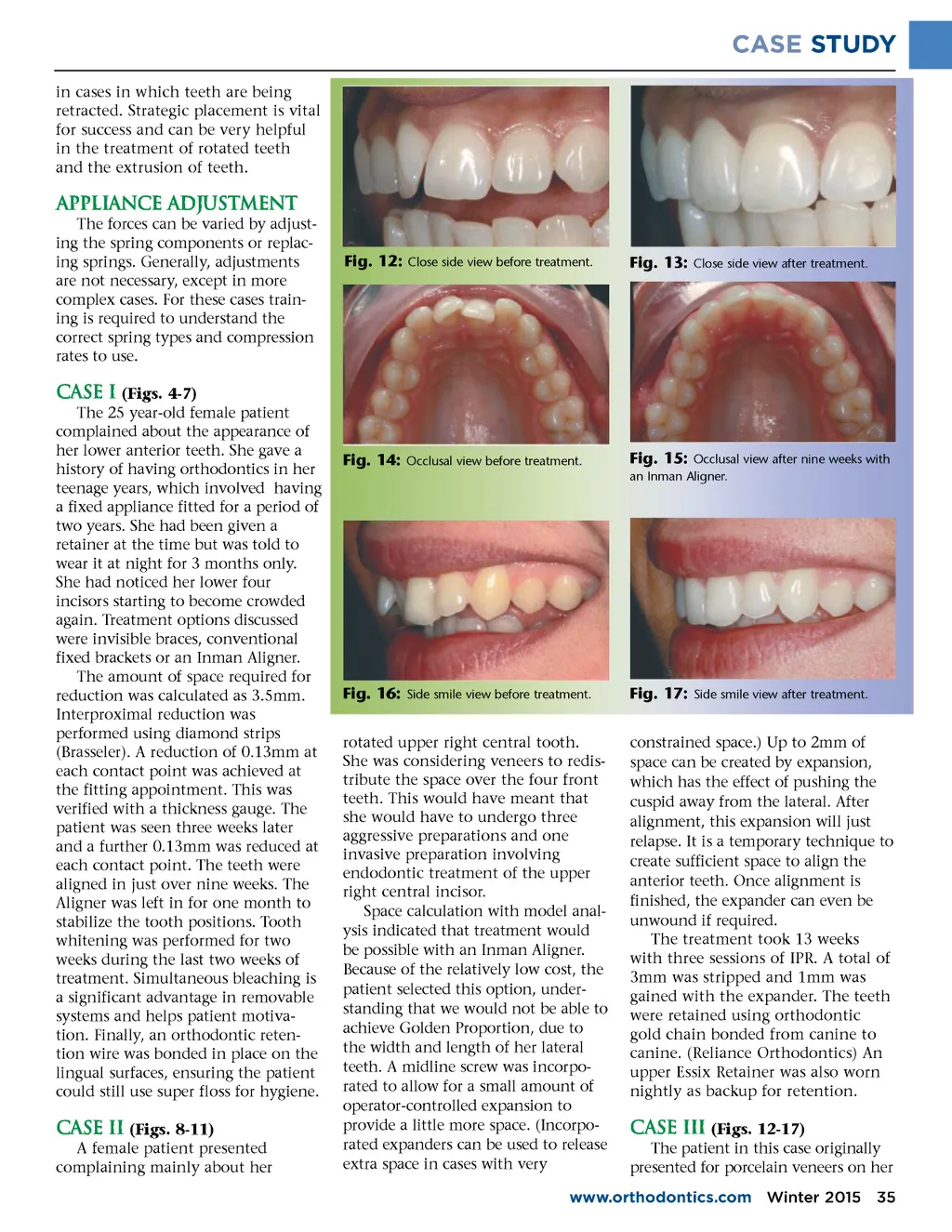
CASE STUDY in cases in which teeth are being retracted. Strategic placement is vital for success and can be very helpful in the treatment of rotated teeth and the extrusion of teeth. Appliance adjustment The forces can be varied by adjust-ing the spring components or replac-ing springs. Generally, adjustments are not necessary, except in more complex cases. For these cases train-ing is required to understand the correct spring types and compression rates to use. Fig. 12: Close side view before treatment. Fig. 13: Close side view after treatment. Case I (Figs. 4-7) The 25 year-old female patient complained about the appearance of her lower anterior teeth. She gave a history of having orthodontics in her teenage years, which involved having a fixed appliance fitted for a period of two years. She had been given a retainer at the time but was told to wear it at night for 3 months only. She had noticed her lower four incisors starting to become crowded again. Treatment options discussed were invisible braces, conventional fixed brackets or an Inman Aligner. The amount of space required for reduction was calculated as 3.5mm. Interproximal reduction was performed using diamond strips (Brasseler). A reduction of 0.13mm at each contact point was achieved at the fitting appointment. This was verified with a thickness gauge. The patient was seen three weeks later and a further 0.13mm was reduced at each contact point. The teeth were aligned in just over nine weeks. The Aligner was left in for one month to stabilize the tooth positions. Tooth whitening was performed for two weeks during the last two weeks of treatment. Simultaneous bleaching is a significant advantage in removable systems and helps patient motiva-tion. Finally, an orthodontic reten-tion wire was bonded in place on the lingual surfaces, ensuring the patient could still use super floss for hygiene. Fig. 14: Occlusal view before treatment. Fig. 15: Occlusal view after nine weeks with an Inman Aligner. Fig. 16: Side smile view before treatment. rotated upper right central tooth. She was considering veneers to redis-tribute the space over the four front teeth. This would have meant that she would have to undergo three aggressive preparations and one invasive preparation involving endodontic treatment of the upper right central incisor. Space calculation with model anal-ysis indicated that treatment would be possible with an Inman Aligner. Because of the relatively low cost, the patient selected this option, under-standing that we would not be able to achieve Golden Proportion, due to the width and length of her lateral teeth. A midline screw was incorpo-rated to allow for a small amount of operator-controlled expansion to provide a little more space. (Incorpo-rated expanders can be used to release extra space in cases with very Fig. 17: Side smile view after treatment. constrained space.) Up to 2mm of space can be created by expansion, which has the effect of pushing the cuspid away from the lateral. After alignment, this expansion will just relapse. It is a temporary technique to create sufficient space to align the anterior teeth. Once alignment is finished, the expander can even be unwound if required. The treatment took 13 weeks with three sessions of IPR. A total of 3mm was stripped and 1mm was gained with the expander. The teeth were retained using orthodontic gold chain bonded from canine to canine. (Reliance Orthodontics) An upper Essix Retainer was also worn nightly as backup for retention. Case II (Figs. 8-11) A female patient presented complaining mainly about her Case III (Figs. 12-17) The patient in this case originally presented for porcelain veneers on her www.orthodontics.com Winter 2015 35
Journal of the American Orthodontic Society Winter 2015: Page 35