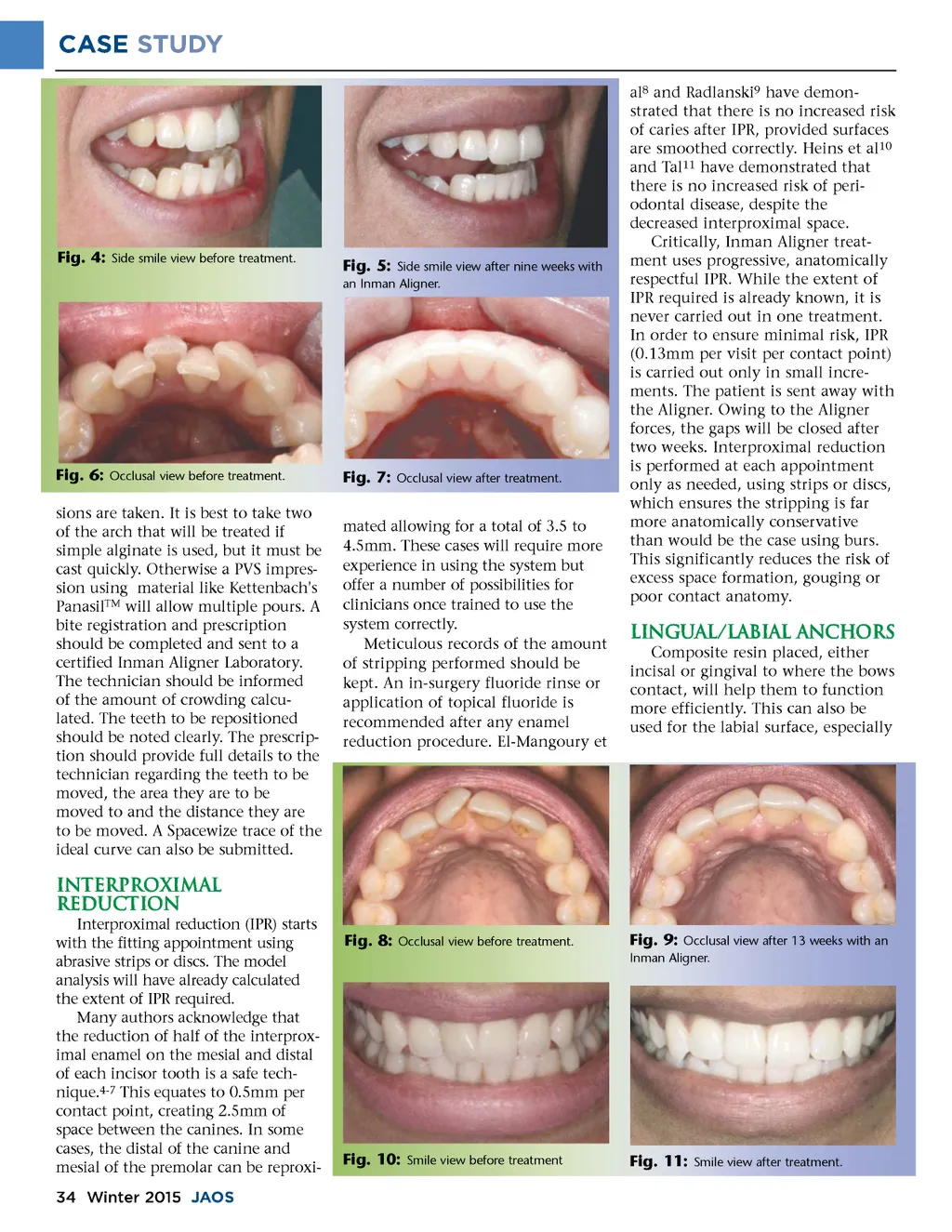
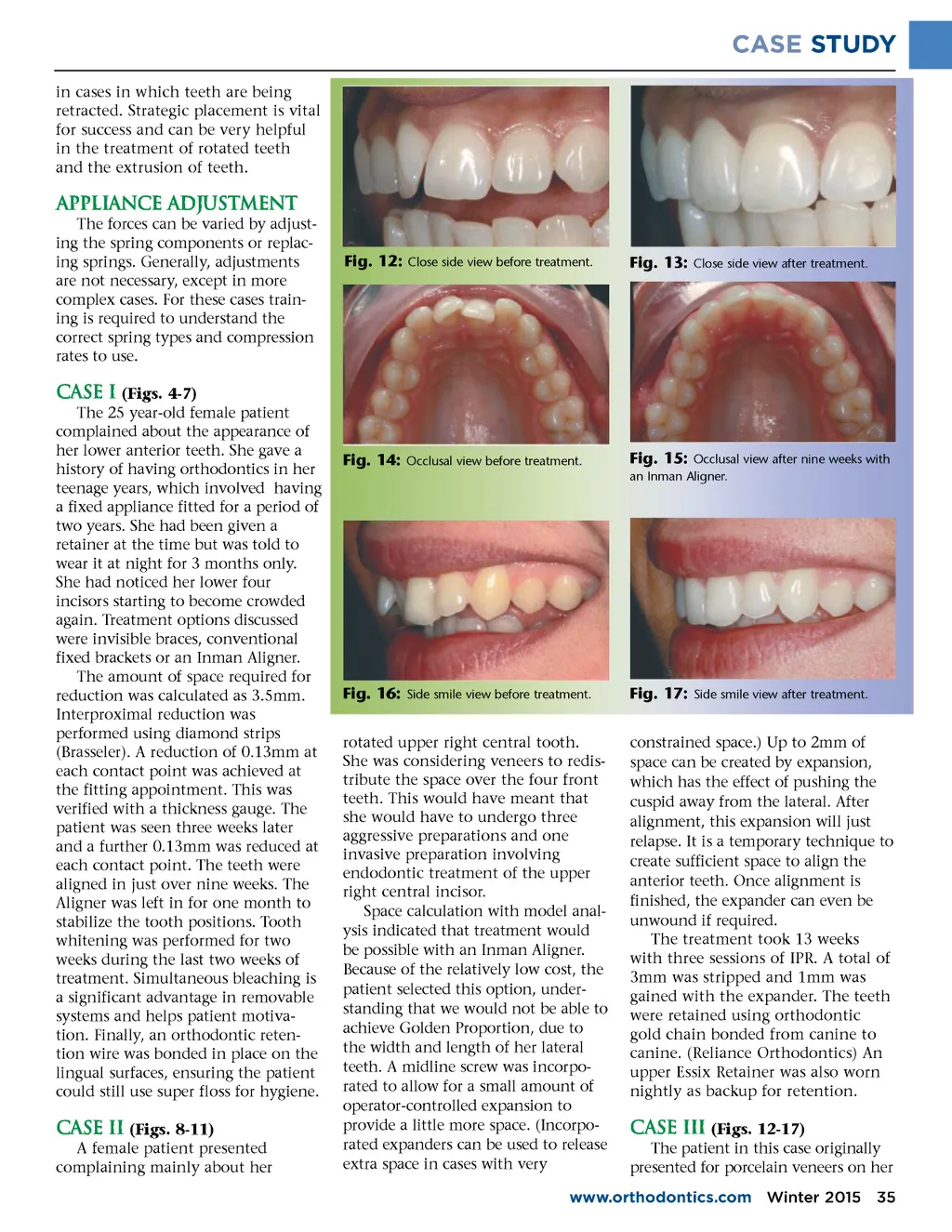
CASE STUDY al 8 and Radlanski 9 have demon-strated that there is no increased risk of caries after IPR, provided surfaces are smoothed correctly. Heins et al 10 and Tal 11 have demonstrated that there is no increased risk of peri-odontal disease, despite the decreased interproximal space. Critically, Inman Aligner treat-ment uses progressive, anatomically respectful IPR. While the extent of IPR required is already known, it is never carried out in one treatment. In order to ensure minimal risk, IPR (0.13mm per visit per contact point) is carried out only in small incre-ments. The patient is sent away with the Aligner. Owing to the Aligner forces, the gaps will be closed after two weeks. Interproximal reduction is performed at each appointment only as needed, using strips or discs, which ensures the stripping is far more anatomically conservative than would be the case using burs. This significantly reduces the risk of excess space formation, gouging or poor contact anatomy. Fig. 4: Side smile view before treatment. Fig. 5: Side smile view after nine weeks with an Inman Aligner. Fig. 6: Occlusal view before treatment. sions are taken. It is best to take two of the arch that will be treated if simple alginate is used, but it must be cast quickly. Otherwise a PVS impres-sion using material like Kettenbach's Panasil TM will allow multiple pours. A bite registration and prescription should be completed and sent to a certified Inman Aligner Laboratory. The technician should be informed of the amount of crowding calcu-lated. The teeth to be repositioned should be noted clearly. The prescrip-tion should provide full details to the technician regarding the teeth to be moved, the area they are to be moved to and the distance they are to be moved. A Spacewize trace of the ideal curve can also be submitted. Fig. 7: Occlusal view after treatment. mated allowing for a total of 3.5 to 4.5mm. These cases will require more experience in using the system but offer a number of possibilities for clinicians once trained to use the system correctly. Meticulous records of the amount of stripping performed should be kept. An in-surgery fluoride rinse or application of topical fluoride is recommended after any enamel reduction procedure. El-Mangoury et Lingual/labial anchors Composite resin placed, either incisal or gingival to where the bows contact, will help them to function more efficiently. This can also be used for the labial surface, especially Interproximal reduction Interproximal reduction (IPR) starts with the fitting appointment using abrasive strips or discs. The model analysis will have already calculated the extent of IPR required. Many authors acknowledge that the reduction of half of the interprox-imal enamel on the mesial and distal of each incisor tooth is a safe tech-nique. 4-7 This equates to 0.5mm per contact point, creating 2.5mm of space between the canines. In some cases, the distal of the canine and mesial of the premolar can be reproxi-34 Winter 2015 JAOS Fig. 8: Occlusal view before treatment. Fig. 9: Occlusal view after 13 weeks with an Inman Aligner. Fig. 10: Smile view before treatment Fig. 11: Smile view after treatment.
Journal of the American Orthodontic Society Winter 2015: Page 34