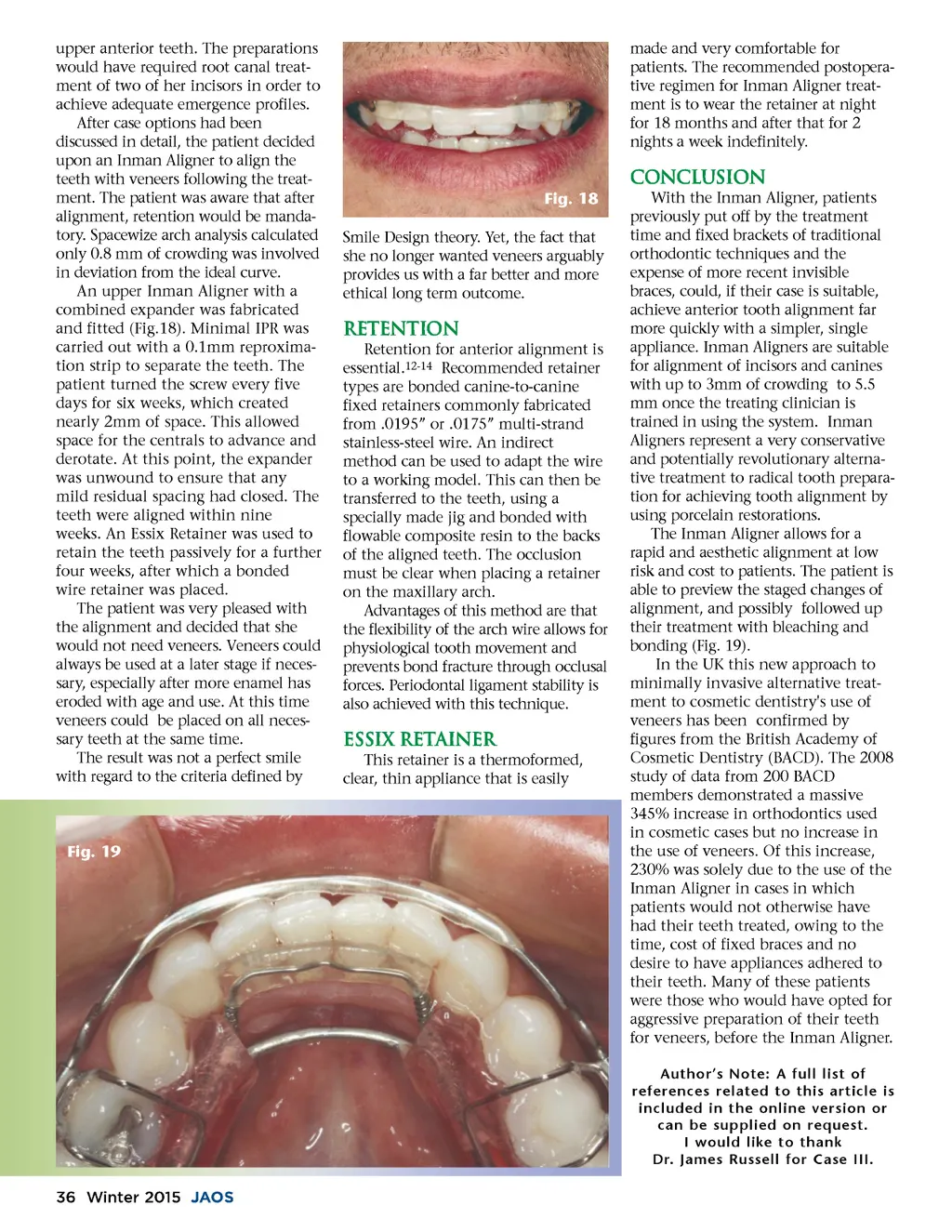
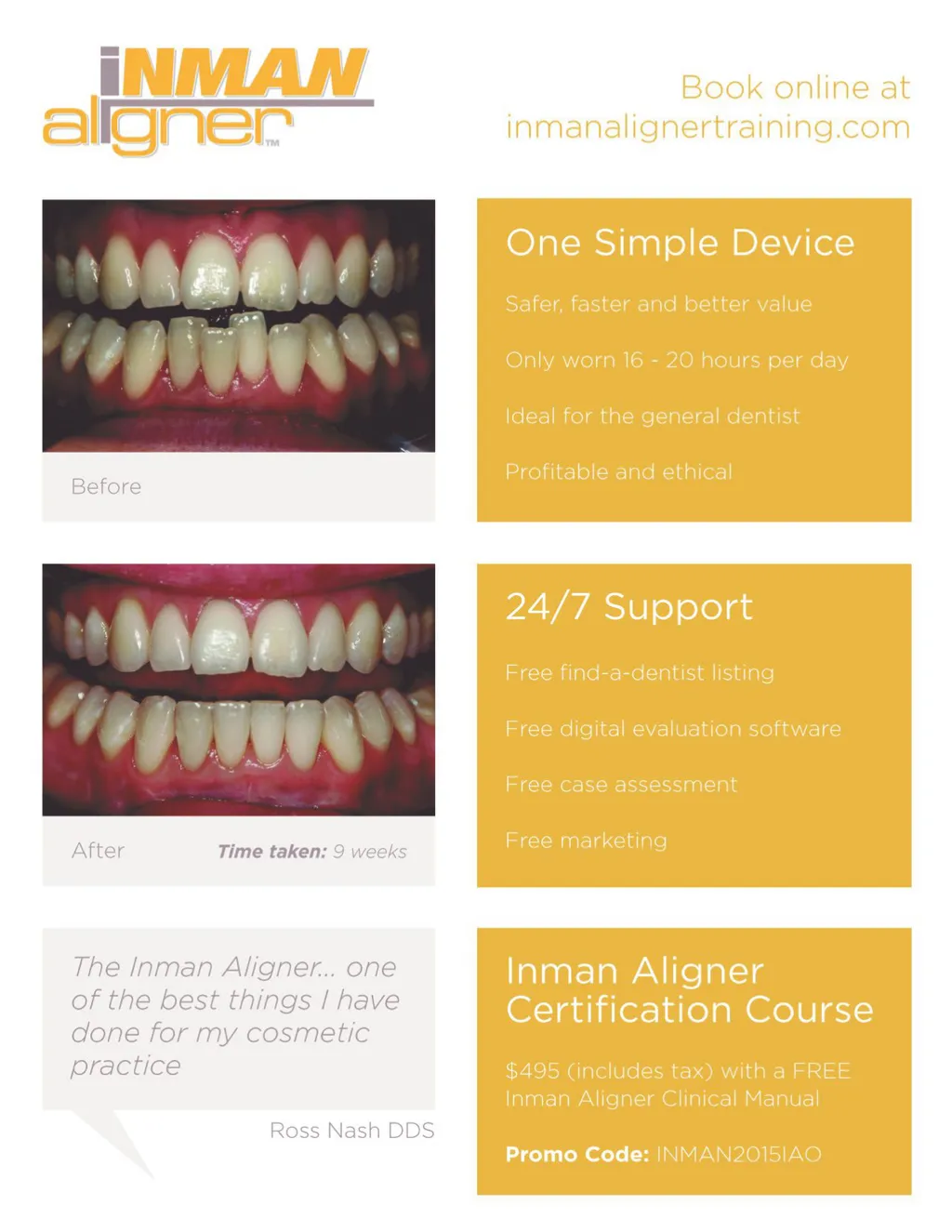
upper anterior teeth. The preparations would have required root canal treat-ment of two of her incisors in order to achieve adequate emergence profiles. After case options had been discussed in detail, the patient decided upon an Inman Aligner to align the teeth with veneers following the treat-ment. The patient was aware that after alignment, retention would be manda-tory. Spacewize arch analysis calculated only 0.8 mm of crowding was involved in deviation from the ideal curve. An upper Inman Aligner with a combined expander was fabricated and fitted (Fig.18). Minimal IPR was carried out with a 0.1mm reproxima-tion strip to separate the teeth. The patient turned the screw every five days for six weeks, which created nearly 2mm of space. This allowed space for the centrals to advance and derotate. At this point, the expander was unwound to ensure that any mild residual spacing had closed. The teeth were aligned within nine weeks. An Essix Retainer was used to retain the teeth passively for a further four weeks, after which a bonded wire retainer was placed. The patient was very pleased with the alignment and decided that she would not need veneers. Veneers could always be used at a later stage if neces-sary, especially after more enamel has eroded with age and use. At this time veneers could be placed on all neces-sary teeth at the same time. The result was not a perfect smile with regard to the criteria defined by made and very comfortable for patients. The recommended postopera-tive regimen for Inman Aligner treat-ment is to wear the retainer at night for 18 months and after that for 2 nights a week indefinitely. Conclusion Fig. 18 Smile Design theory. Yet, the fact that she no longer wanted veneers arguably provides us with a far better and more ethical long term outcome. With the Inman Aligner, patients previously put off by the treatment time and fixed brackets of traditional orthodontic techniques and the expense of more recent invisible braces, could, if their case is suitable, achieve anterior tooth alignment far more quickly with a simpler, single appliance. Inman Aligners are suitable for alignment of incisors and canines with up to 3mm of crowding to 5.5 mm once the treating clinician is trained in using the system. Inman Aligners represent a very conservative and potentially revolutionary alterna-tive treatment to radical tooth prepara-tion for achieving tooth alignment by using porcelain restorations. The Inman Aligner allows for a rapid and aesthetic alignment at low risk and cost to patients. The patient is able to preview the staged changes of alignment, and possibly followed up their treatment with bleaching and bonding (Fig. 19). In the UK this new approach to minimally invasive alternative treat-ment to cosmetic dentistry's use of veneers has been confirmed by figures from the British Academy of Cosmetic Dentistry (BACD). The 2008 study of data from 200 BACD members demonstrated a massive 345% increase in orthodontics used in cosmetic cases but no increase in the use of veneers. Of this increase, 230% was solely due to the use of the Inman Aligner in cases in which patients would not otherwise have had their teeth treated, owing to the time, cost of fixed braces and no desire to have appliances adhered to their teeth. Many of these patients were those who would have opted for aggressive preparation of their teeth for veneers, before the Inman Aligner. Author’s Note: A full list of references related to this article is included in the online version or can be supplied on request. I would like to thank Dr. James Russell for Case III. R etention Retention for anterior alignment is essential. 12-14 Recommended retainer types are bonded canine-to-canine fixed retainers commonly fabricated from .0195” or .0175” multi-strand stainless-steel wire. An indirect method can be used to adapt the wire to a working model. This can then be transferred to the teeth, using a specially made jig and bonded with flowable composite resin to the backs of the aligned teeth. The occlusion must be clear when placing a retainer on the maxillary arch. Advantages of this method are that the flexibility of the arch wire allows for physiological tooth movement and prevents bond fracture through occlusal forces. Periodontal ligament stability is also achieved with this technique. Essix Retainer This retainer is a thermoformed, clear, thin appliance that is easily Fig. 19 36 Winter 2015 JAOS
Journal of the American Orthodontic Society Winter 2015: Page 36