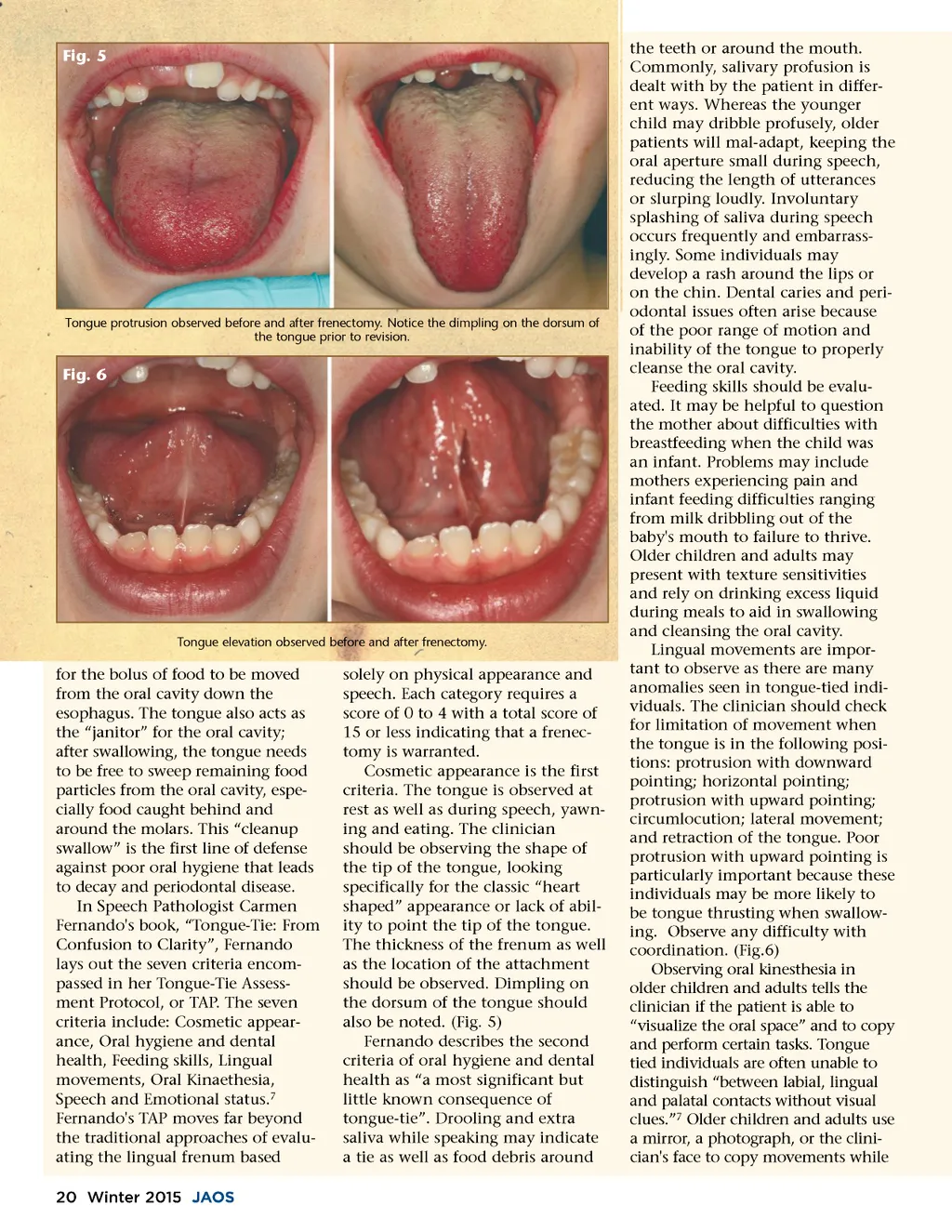
Fig. 5 Tongue protrusion observed before and after frenectomy. Notice the dimpling on the dorsum of the tongue prior to revision. Fig. 6 Tongue elevation observed before and after frenectomy. for the bolus of food to be moved from the oral cavity down the esophagus. The tongue also acts as the “janitor” for the oral cavity; after swallowing, the tongue needs to be free to sweep remaining food particles from the oral cavity, espe-cially food caught behind and around the molars. This “clean up swallow” is the first line of defense against poor oral hygiene that leads to decay and periodontal disease. In Speech Pathologist Carmen Fernando's book, “Tongue-Tie: From Confusion to Clarity”, Fernando lays out the seven criteria encom-passed in her Tongue-Tie Assess-ment Protocol, or TAP. The seven criteria include: Cosmetic appear-ance, Oral hygiene and dental health, Feeding skills, Lingual movements, Oral Kinaethesia, Speech and Emotional status. 7 Fernando's TAP moves far beyond the traditional approaches of evalu-ating the lingual frenum based 20 Winter 2015 JAOS solely on physical appearance and speech. Each category requires a score of 0 to 4 with a total score of 15 or less indicating that a frenec-tomy is warranted. Cosmetic appearance is the first criteria. The tongue is observed at rest as well as during speech, yawn-ing and eating. The clinician should be observing the shape of the tip of the tongue, looking specifically for the classic “heart shaped” appearance or lack of abil-ity to point the tip of the tongue. The thickness of the frenum as well as the location of the attachment should be observed. Dimpling on the dorsum of the tongue should also be noted. (Fig. 5) Fernando describes the second criteria of oral hygiene and dental health as “a most significant but little known consequence of tongue-tie”. Drooling and extra saliva while speaking may indicate a tie as well as food debris around the teeth or around the mouth. Commonly, salivary profusion is dealt with by the patient in differ-ent ways. Whereas the younger child may dribble profusely, older patients will mal-adapt, keeping the oral aperture small during speech, reducing the length of utterances or slurping loudly. Involuntary splashing of saliva during speech occurs frequently and embarrass-ingly. Some individuals may develop a rash around the lips or on the chin. Dental caries and peri-odontal issues often arise because of the poor range of motion and inability of the tongue to properly cleanse the oral cavity. Feeding skills should be evalu-ated. It may be helpful to question the mother about difficulties with breastfeeding when the child was an infant. Problems may include mothers experiencing pain and infant feeding difficulties ranging from milk dribbling out of the baby's mouth to failure to thrive. Older children and adults may present with texture sensitivities and rely on drinking excess liquid during meals to aid in swallowing and cleansing the oral cavity. Lingual movements are impor-tant to observe as there are many anomalies seen in tongue-tied indi-viduals. The clinician should check for limitation of movement when the tongue is in the following posi-tions: protrusion with downward pointing; horizontal pointing; protrusion with upward pointing; circumlocution; lateral movement; and retraction of the tongue. Poor protrusion with upward pointing is particularly important because these individuals may be more likely to be tongue thrusting when swallow-ing. Observe any difficulty with coordination. (Fig.6) Observing oral kinesthesia in older children and adults tells the clinician if the patient is able to “visualize the oral space” and to copy and perform certain tasks. Tongue tied individuals are often unable to distinguish “between labial, lingual and palatal contacts without visual clues.” 7 Older children and adults use a mirror, a photograph, or the clini-cian's face to copy movements while
Journal of the American Orthodontic Society Winter 2015: Page 20