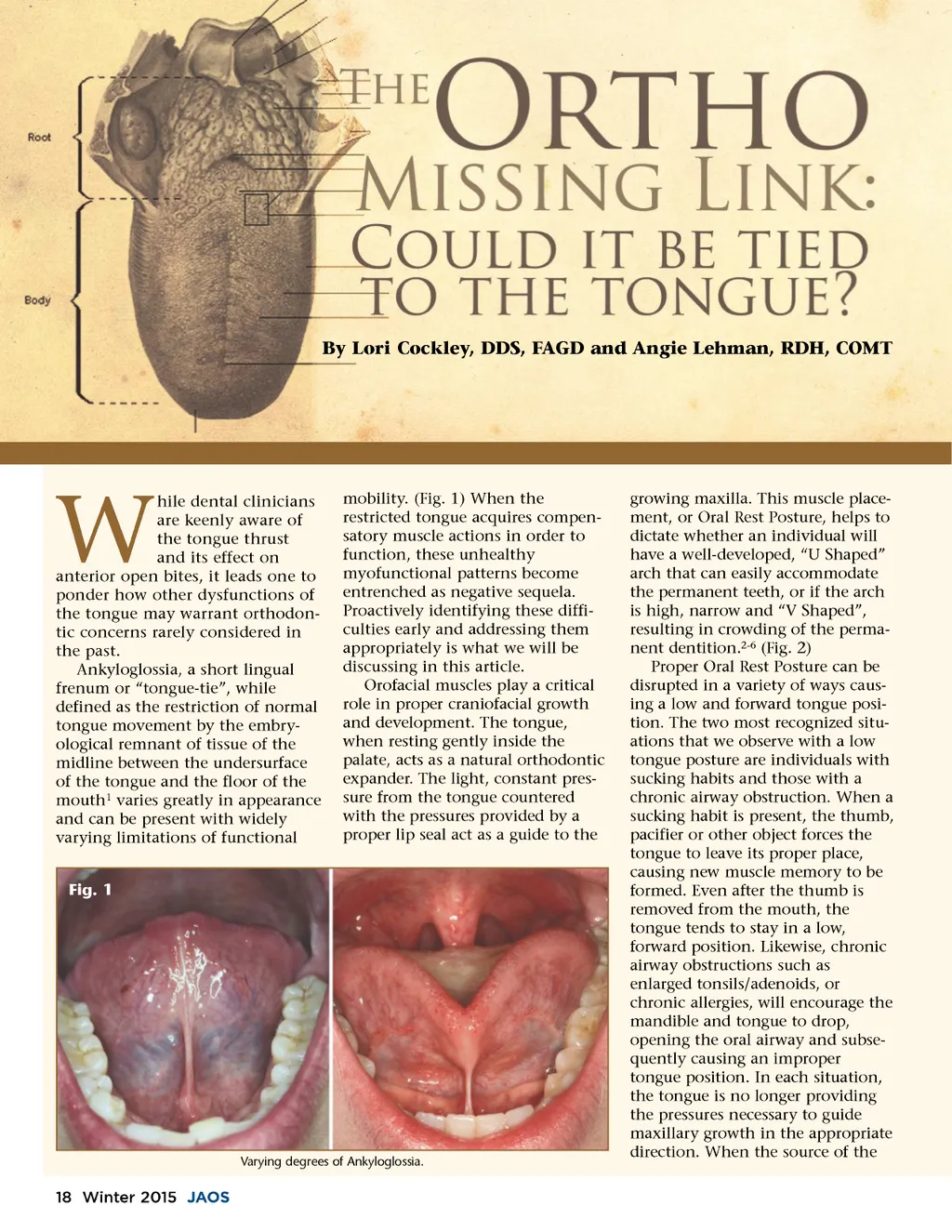
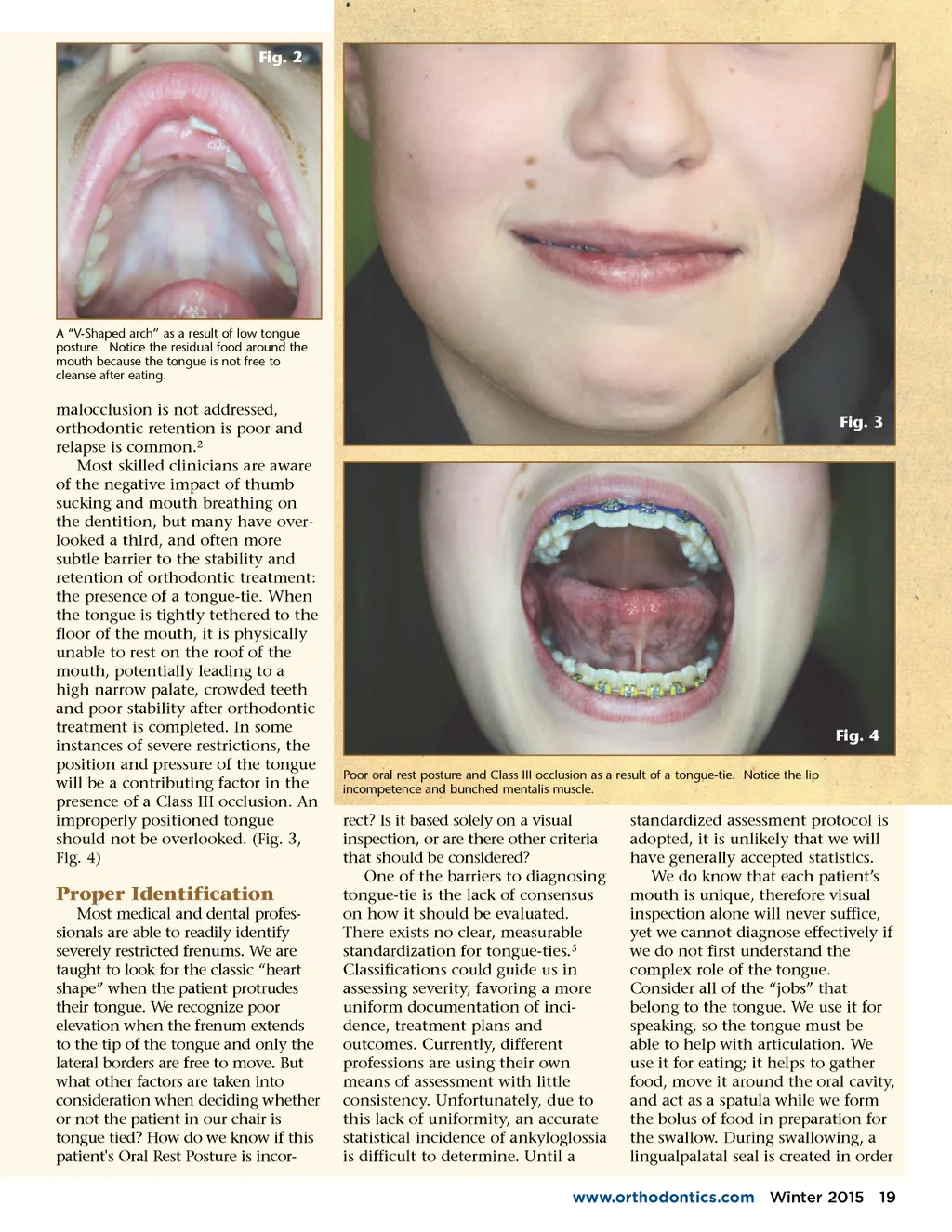
Fig. 2 A “V-Shaped arch” as a result of low tongue posture. Notice the residual food around the mouth because the tongue is not free to cleanse after eating. malocclusion is not addressed, orthodontic retention is poor and relapse is common. 2 Most skilled clinicians are aware of the negative impact of thumb sucking and mouth breathing on the dentition, but many have over-looked a third, and often more subtle barrier to the stability and retention of orthodontic treatment: the presence of a tongue-tie. When the tongue is tightly tethered to the floor of the mouth, it is physically unable to rest on the roof of the mouth, potentially leading to a high narrow palate, crowded teeth and poor stability after orthodontic treatment is completed. In some instances of severe restrictions, the position and pressure of the tongue will be a contributing factor in the presence of a Class III occlusion. An improperly positioned tongue should not be overlooked. (Fig. 3, Fig. 4) Fig. 3 Fig. 4 Poor oral rest posture and Class III occlusion as a result of a tongue-tie. Notice the lip incompetence and bunched mentalis muscle. Proper Identification Most medical and dental profes-sionals are able to readily identify severely restricted frenums. We are taught to look for the classic “heart shape” when the patient protrudes their tongue. We recognize poor elevation when the frenum extends to the tip of the tongue and only the lateral borders are free to move. But what other factors are taken into consideration when deciding whether or not the patient in our chair is tongue tied? How do we know if this patient's Oral Rest Posture is incor-rect? Is it based solely on a visual inspection, or are there other criteria that should be considered? One of the barriers to diagnosing tongue-tie is the lack of consensus on how it should be evaluated. There exists no clear, measurable standardization for tongue-ties. 5 Classifications could guide us in assessing severity, favoring a more uniform documentation of inci-dence, treatment plans and outcomes. Currently, different professions are using their own means of assessment with little consistency. Unfortunately, due to this lack of uniformity, an accurate statistical incidence of ankyloglossia is difficult to determine. Until a standardized assessment protocol is adopted, it is unlikely that we will have generally accepted statistics. We do know that each patient’s mouth is unique, therefore visual inspection alone will never suffice, yet we cannot diagnose effectively if we do not first understand the complex role of the tongue. Consider all of the “jobs” that belong to the tongue. We use it for speaking, so the tongue must be able to help with articulation. We use it for eating; it helps to gather food, move it around the oral cavity, and act as a spatula while we form the bolus of food in preparation for the swallow. During swallowing, a lingual palatal seal is created in order www.orthodontics.com Winter 2015 19
Journal of the American Orthodontic Society Winter 2015: Page 19