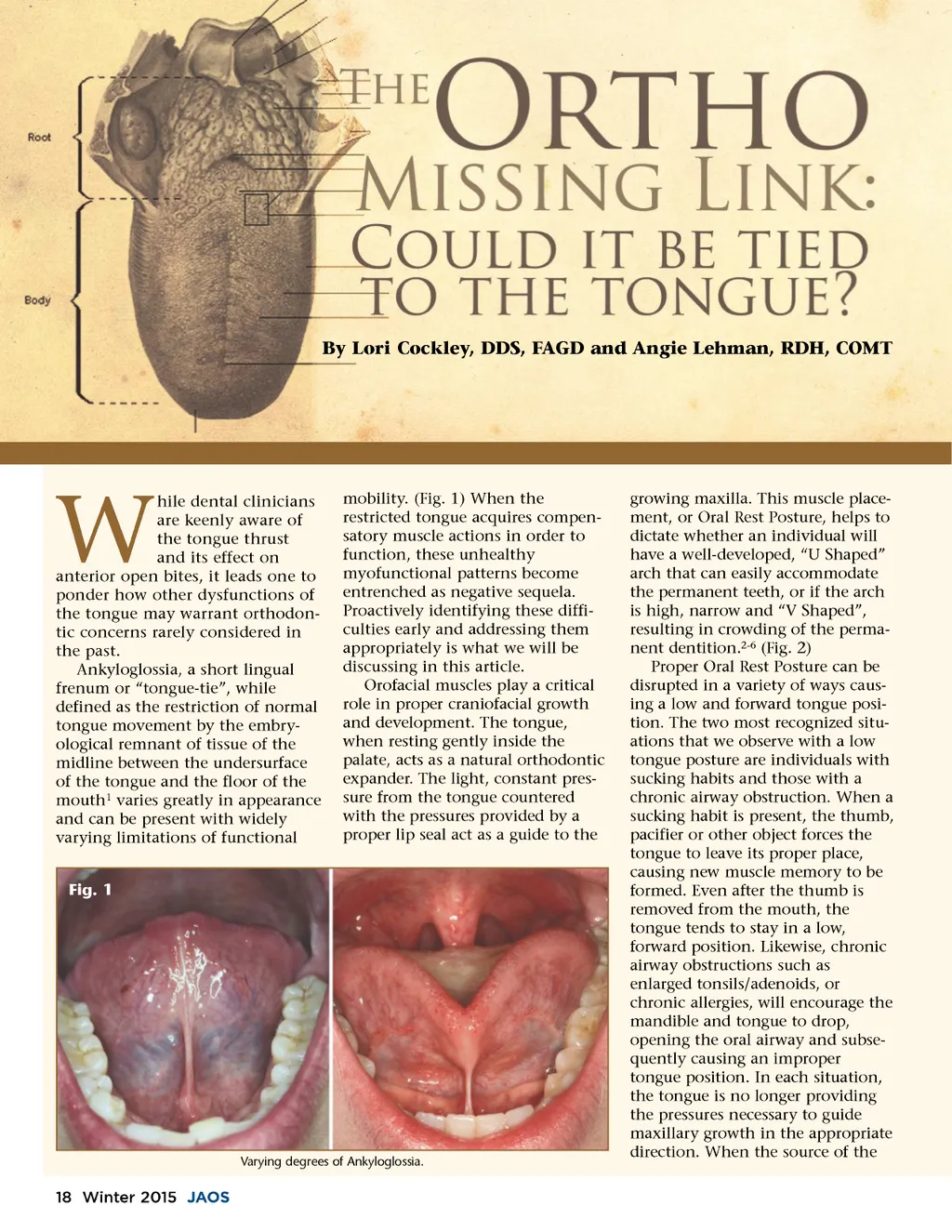
By Lori Cockley, DDS, FAGD and Angie Lehman, RDH, COMT W hile dental clinicians are keenly aware of the tongue thrust and its effect on anterior open bites, it leads one to ponder how other dysfunctions of the tongue may warrant orthodon-tic concerns rarely considered in the past. Ankyloglossia, a short lingual frenum or “tongue-tie”, while defined as the restriction of normal tongue movement by the embry-ological remnant of tissue of the midline between the undersurface of the tongue and the floor of the mouth 1 varies greatly in appearance and can be present with widely varying limitations of functional Fig. 1 mobility. (Fig. 1) When the restricted tongue acquires compen-satory muscle actions in order to function, these unhealthy myofunctional patterns become entrenched as negative sequela. Proactively identifying these diffi-culties early and addressing them appropriately is what we will be discussing in this article. Orofacial muscles play a critical role in proper craniofacial growth and development. The tongue, when resting gently inside the palate, acts as a natural orthodontic expander. The light, constant pres-sure from the tongue countered with the pressures provided by a proper lip seal act as a guide to the Varying degrees of Ankyloglossia. growing maxilla. This muscle place-ment, or Oral Rest Posture, helps to dictate whether an individual will have a well-developed, “U Shaped” arch that can easily accommodate the permanent teeth, or if the arch is high, narrow and “V Shaped”, resulting in crowding of the perma-nent dentition. 2-6 (Fig. 2) Proper Oral Rest Posture can be disrupted in a variety of ways caus-ing a low and forward tongue posi-tion. The two most recognized situ-ations that we observe with a low tongue posture are individuals with sucking habits and those with a chronic airway obstruction. When a sucking habit is present, the thumb, pacifier or other object forces the tongue to leave its proper place, causing new muscle memory to be formed. Even after the thumb is removed from the mouth, the tongue tends to stay in a low, forward position. Likewise, chronic airway obstructions such as enlarged tonsils/adenoids, or chronic allergies, will encourage the mandible and tongue to drop, opening the oral airway and subse-quently causing an improper tongue position. In each situation, the tongue is no longer providing the pressures necessary to guide maxillary growth in the appropriate direction. When the source of the 18 Winter 2015 JAOS
Journal of the American Orthodontic Society Winter 2015: Page 18