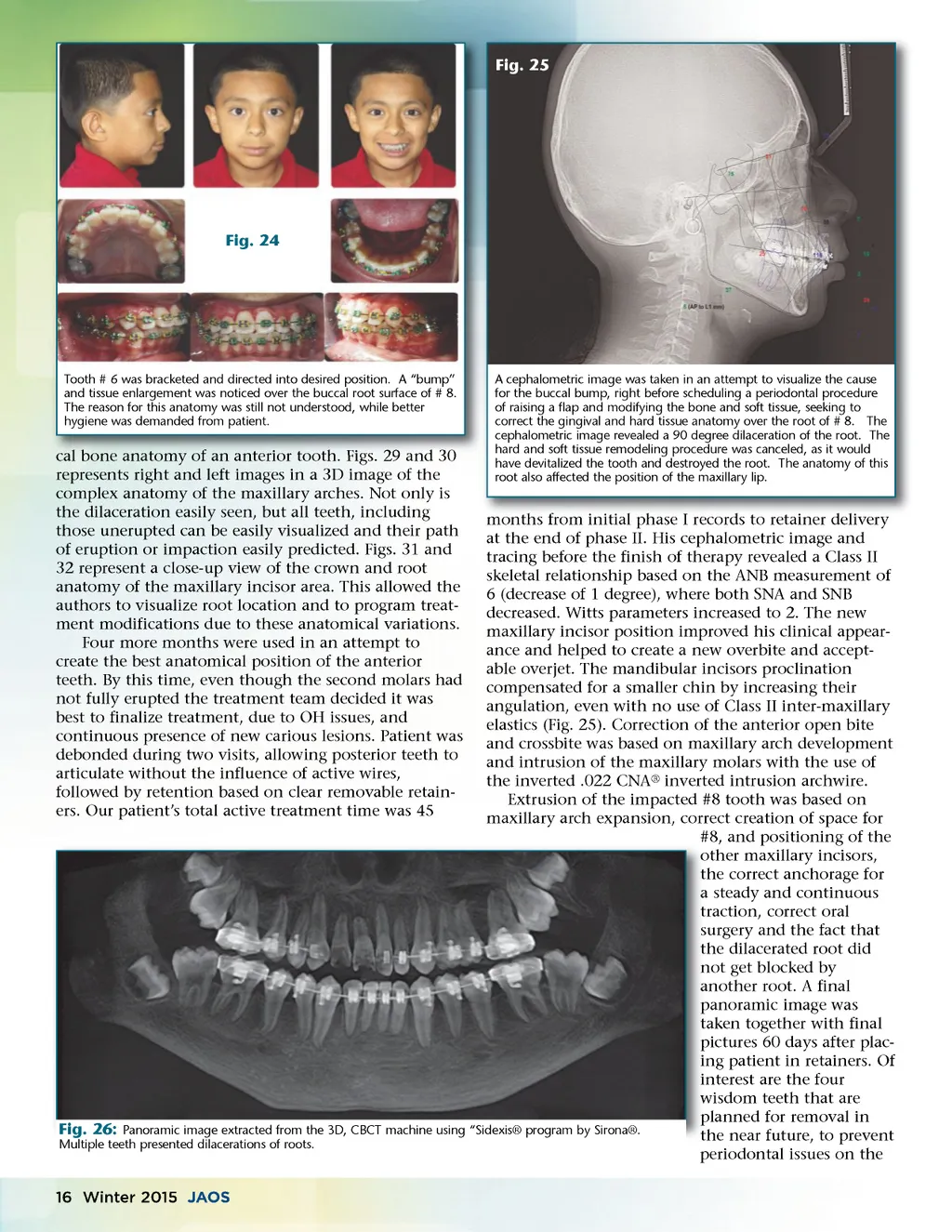
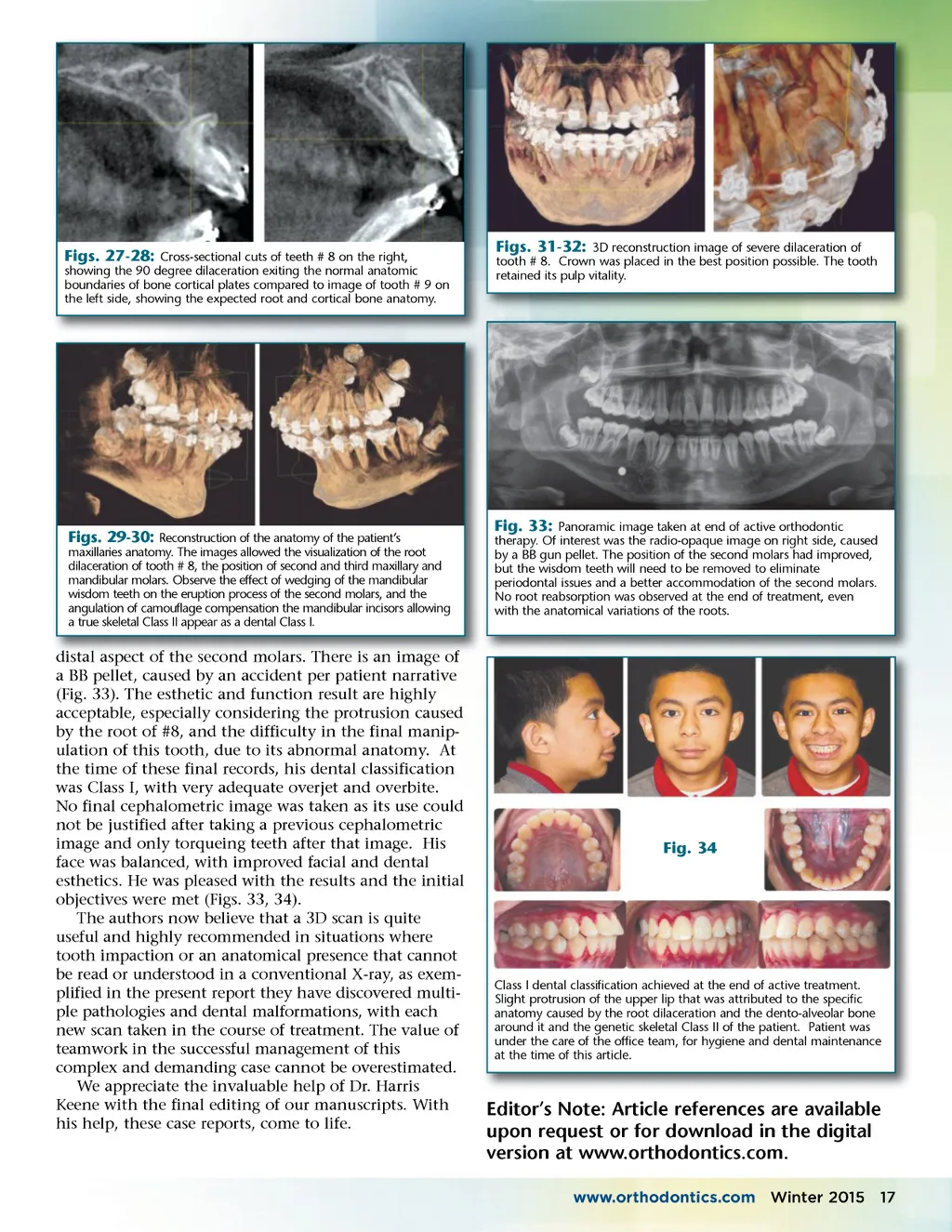
Figs. 27-28: Cross-sectional cuts of teeth # 8 on the right, showing the 90 degree dilaceration exiting the normal anatomic boundaries of bone cortical plates compared to image of tooth # 9 on the left side, showing the expected root and cortical bone anatomy. Figs. 31-32: 3D reconstruction image of severe dilaceration of tooth # 8. Crown was placed in the best position possible. The tooth retained its pulp vitality. Figs. 29-30: Reconstruction of the anatomy of the patient’s maxillaries anatomy. The images allowed the visualization of the root dilaceration of tooth # 8, the position of second and third maxillary and mandibular molars. Observe the effect of wedging of the mandibular wisdom teeth on the eruption process of the second molars, and the angulation of camouflage compensation the mandibular incisors allowing a true skeletal Class II appear as a dental Class I. Fig. 33: Panoramic image taken at end of active orthodontic therapy. Of interest was the radio-opaque image on right side, caused by a BB gun pellet. The position of the second molars had improved, but the wisdom teeth will need to be removed to eliminate periodontal issues and a better accommodation of the second molars. No root reabsorption was observed at the end of treatment, even with the anatomical variations of the roots. distal aspect of the second molars molars. There is an image of a BB pellet, caused by an accident per patient narrative (Fig. 33). The esthetic and function result are highly acceptable, especially considering the protrusion caused by the root of #8, and the difficulty in the final manip-ulation of this tooth, due to its abnormal anatomy. At the time of these final records, his dental classification was Class I, with very adequate overjet and overbite. No final cephalometric image was taken as its use could not be justified after taking a previous cephalometric image and only torqueing teeth after that image. His face was balanced, with improved facial and dental esthetics. He was pleased with the results and the initial objectives were met (Figs. 33, 34). The authors now believe that a 3D scan is quite useful and highly recommended in situations where tooth impaction or an anatomical presence that cannot be read or understood in a conventional X-ray, as exem-plified in the present report they have discovered multi-ple pathologies and dental malformations, with each new scan taken in the course of treatment. The value of teamwork in the successful management of this complex and demanding case cannot be overestimated. We appreciate the invaluable help of Dr. Harris Keene with the final editing of our manuscripts. With his help, these case reports, come to life. Fig. 34 Class I dental classification achieved at the end of active treatment. Slight protrusion of the upper lip that was attributed to the specific anatomy caused by the root dilaceration and the dento-alveolar bone around it and the genetic skeletal Class II of the patient. Patient was under the care of the office team, for hygiene and dental maintenance at the time of this article. Editor’s Note: Article references are available upon request or for download in the digital version at www.orthodontics.com. www.orthodontics.com Winter 2015 17
Journal of the American Orthodontic Society Winter 2015: Page 17