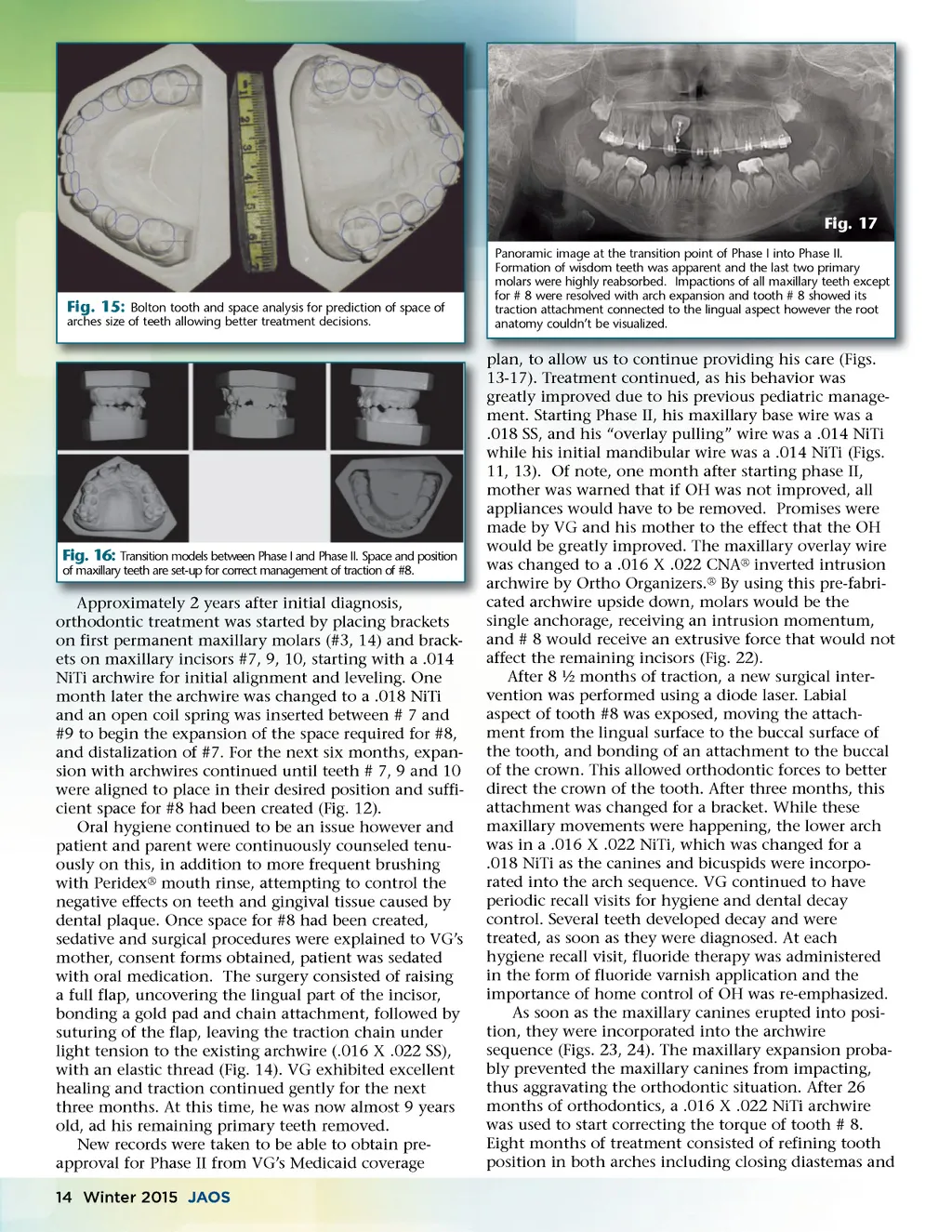
Fig. 17 Panoramic image at the transition point of Phase I into Phase II. Formation of wisdom teeth was apparent and the last two primary molars were highly reabsorbed. Impactions of all maxillary teeth except for # 8 were resolved with arch expansion and tooth # 8 showed its traction attachment connected to the lingual aspect however the root anatomy couldn’t be visualized. Fig. 15: Bolton tooth and space analysis for prediction of space of arches size of teeth allowing better treatment decisions. Fig. 16: Transition models between Phase I and Phase II. Space and position of maxillary teeth are set-up for correct management of traction of #8. diagnosis, Approximately 2 years after initial diagnosis orthodontic treatment was started by placing brackets on first permanent maxillary molars (#3, 14) and brack-ets on maxillary incisors #7, 9, 10, starting with a .014 NiTi archwire for initial alignment and leveling. One month later the archwire was changed to a .018 NiTi and an open coil spring was inserted between # 7 and #9 to begin the expansion of the space required for #8, and distalization of #7. For the next six months, expan-sion with archwires continued until teeth # 7, 9 and 10 were aligned to place in their desired position and suffi-cient space for #8 had been created (Fig. 12). Oral hygiene continued to be an issue however and patient and parent were continuously counseled tenu-ously on this, in addition to more frequent brushing with Peridex ® mouth rinse, attempting to control the negative effects on teeth and gingival tissue caused by dental plaque. Once space for #8 had been created, sedative and surgical procedures were explained to VG’s mother, consent forms obtained, patient was sedated with oral medication. The surgery consisted of raising a full flap, uncovering the lingual part of the incisor, bonding a gold pad and chain attachment, followed by suturing of the flap, leaving the traction chain under light tension to the existing archwire (.016 X .022 SS), with an elastic thread (Fig. 14). VG exhibited excellent healing and traction continued gently for the next three months. At this time, he was now almost 9 years old, ad his remaining primary teeth removed. New records were taken to be able to obtain pre-approval for Phase II from VG’s Medicaid coverage 14 Winter 2015 JAOS plan, to allow us to continue providing his care (Figs (Figs. plan 13-17). Treatment continued, as his behavior was greatly improved due to his previous pediatric manage-ment. Starting Phase II, his maxillary base wire was a .018 SS, and his “overlay pulling” wire was a .014 NiTi while his initial mandibular wire was a .014 NiTi (Figs. 11, 13). Of note, one month after starting phase II, mother was warned that if OH was not improved, all appliances would have to be removed. Promises were made by VG and his mother to the effect that the OH would be greatly improved. The maxillary overlay wire was changed to a .016 X .022 CNA ® inverted intrusion archwire by Ortho Organizers. ® By using this pre-fabri-cated archwire upside down, molars would be the single anchorage, receiving an intrusion momentum, and # 8 would receive an extrusive force that would not affect the remaining incisors (Fig. 22). After 8 ½ months of traction, a new surgical inter-vention was performed using a diode laser. Labial aspect of tooth #8 was exposed, moving the attach-ment from the lingual surface to the buccal surface of the tooth, and bonding of an attachment to the buccal of the crown. This allowed orthodontic forces to better direct the crown of the tooth. After three months, this attachment was changed for a bracket. While these maxillary movements were happening, the lower arch was in a .016 X .022 NiTi, which was changed for a .018 NiTi as the canines and bicuspids were incorpo-rated into the arch sequence. VG continued to have periodic recall visits for hygiene and dental decay control. Several teeth developed decay and were treated, as soon as they were diagnosed. At each hygiene recall visit, fluoride therapy was administered in the form of fluoride varnish application and the importance of home control of OH was re-emphasized. As soon as the maxillary canines erupted into posi-tion, they were incorporated into the archwire sequence (Figs. 23, 24). The maxillary expansion proba-bly prevented the maxillary canines from impacting, thus aggravating the orthodontic situation. After 26 months of orthodontics, a .016 X .022 NiTi archwire was used to start correcting the torque of tooth # 8. Eight months of treatment consisted of refining tooth position in both arches including closing diastemas and
Journal of the American Orthodontic Society Winter 2015: Page 14