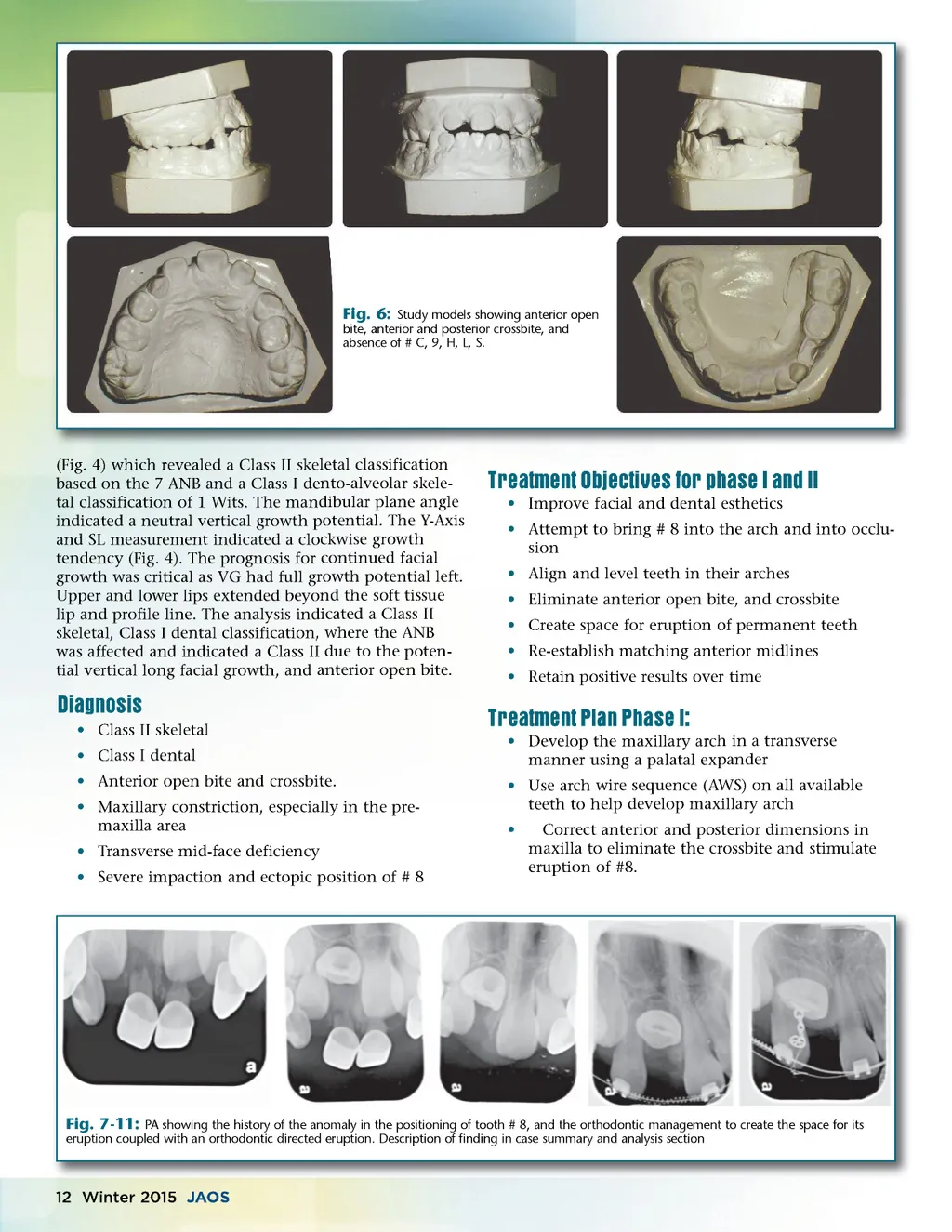
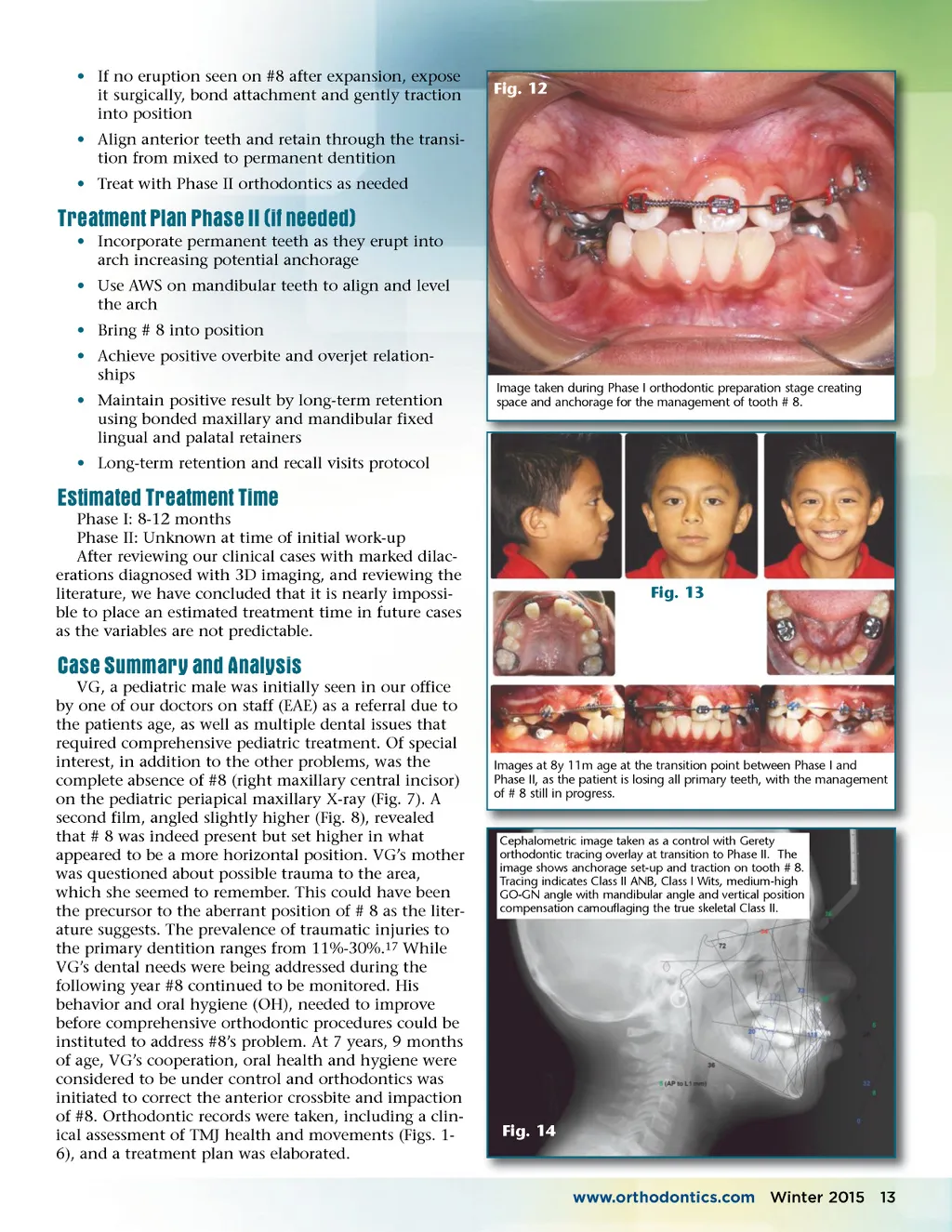
• If no eruption seen on #8 after expansion, expose it surgically, bond attachment and gently traction into position • Align anterior teeth and retain through the transi-tion from mixed to permanent dentition • Treat with Phase II orthodontics as needed Fig. 12 Treatment Plan Phase II (if needed) • Incorporate permanent teeth as they erupt into arch increasing potential anchorage • Use AWS on mandibular teeth to align and level the arch • Bring # 8 into position • Achieve positive overbite and overjet relation-ships • Maintain positive result by long-term retention using bonded maxillary and mandibular fixed lingual and palatal retainers • Long-term retention and recall visits protocol Image taken during Phase I orthodontic preparation stage creating space and anchorage for the management of tooth # 8. Estimated Treatment Time Phase I: 8-12 months Phase II: Unknown at time of initial work-up After reviewing our clinical cases with marked dilac-erations diagnosed with 3D imaging, and reviewing the literature, we have concluded that it is nearly impossi-ble to place an estimated treatment time in future cases as the variables are not predictable. Fig. 13 Case Summary and Analysis VG, a pediatric male was initially seen in our office by one of our doctors on staff (EAE) as a referral due to the patients age, as well as multiple dental issues that required comprehensive pediatric treatment. Of special interest, in addition to the other problems, was the complete absence of #8 (right maxillary central incisor) on the pediatric periapical maxillary X-ray (Fig. 7). A second film, angled slightly higher (Fig. 8), revealed that # 8 was indeed present but set higher in what appeared to be a more horizontal position. VG’s mother was questioned about possible trauma to the area, which she seemed to remember. This could have been the precursor to the aberrant position of # 8 as the liter-ature suggests. The prevalence of traumatic injuries to the primary dentition ranges from 11%-30%. 17 While VG’s dental needs were being addressed during the following year #8 continued to be monitored. His behavior and oral hygiene (OH), needed to improve before comprehensive orthodontic procedures could be instituted to address #8’s problem. At 7 years, 9 months of age, VG’s cooperation, oral health and hygiene were considered to be under control and orthodontics was initiated to correct the anterior crossbite and impaction of #8. Orthodontic records were taken, including a clin-ical assessment of TMJ health and movements (Figs. 1-6), and a treatment plan was elaborated. Images at 8y 11m age at the transition point between Phase I and Phase II, as the patient is losing all primary teeth, with the management of # 8 still in progress. Cephalometric image taken as a control with Gerety orthodontic tracing overlay at transition to Phase II. The image shows anchorage set-up and traction on tooth # 8. Tracing indicates Class II ANB, Class I Wits, medium-high GO-GN angle with mandibular angle and vertical position compensation camouflaging the true skeletal Class II. Fig. 14 www.orthodontics.com Winter 2015 13
Journal of the American Orthodontic Society Winter 2015: Page 13