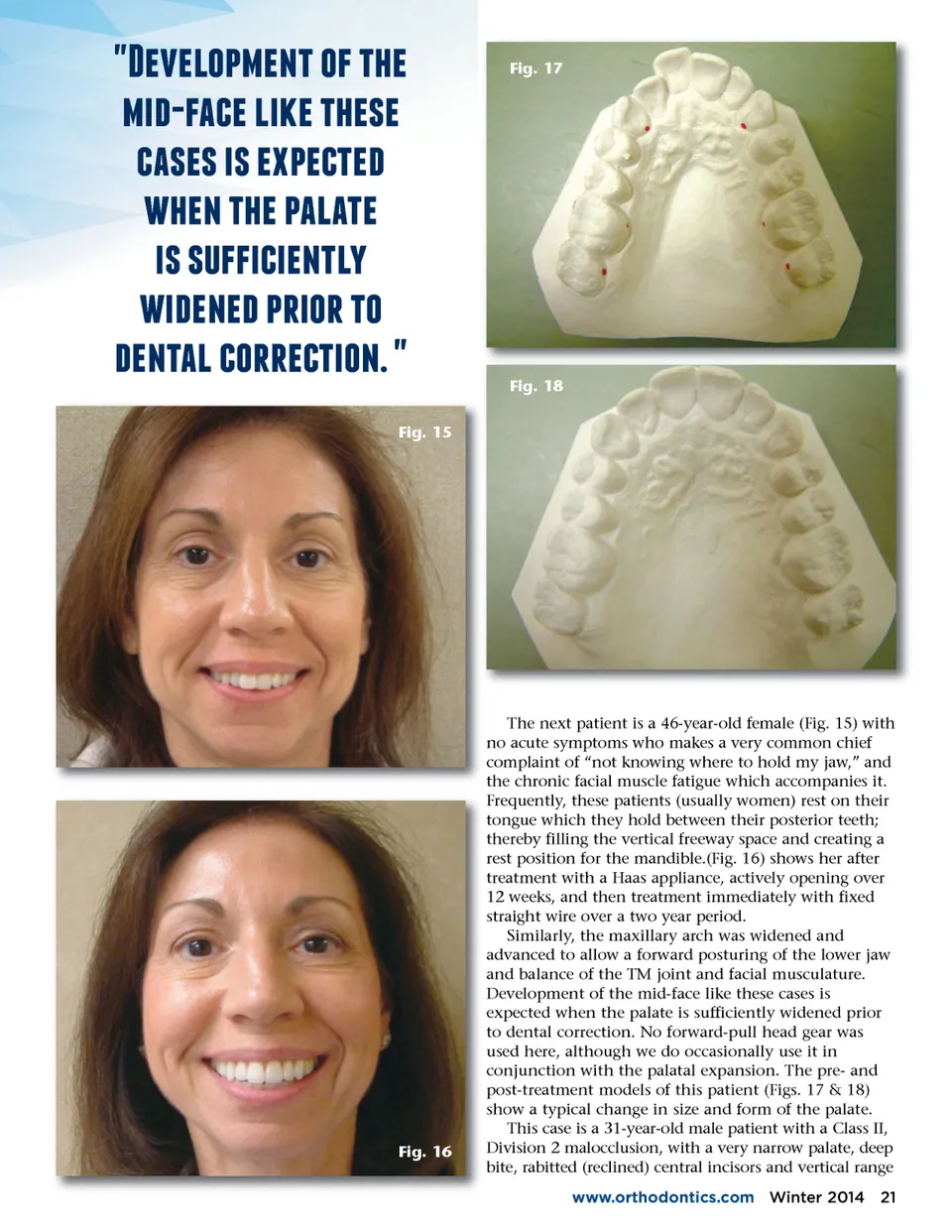
f;66,/#6257/$75%6 4)$3(67,4675%616 (316174176#6(56) %6275%67#3,356 4171 $$4(4625, 4)626)7#*4/*75/ )6253,7(/**6(54/2 7 Fig. 15 Fig. 17 Fig. 18 Fig. 16 The next patient is a 46-year-old female (Fig. 15) with no acute symptoms who makes a very common chief complaint of “not knowing where to hold my jaw,” and the chronic facial muscle fatigue which accompanies it. Frequently, these patients (usually women) rest on their tongue which they hold between their posterior teeth; thereby filling the vertical freeway space and creating a rest position for the mandible.(Fig. 16) shows her after treatment with a Haas appliance, actively opening over 12 weeks, and then treatment immediately with fixed straight wire over a two year period. Similarly, the maxillary arch was widened and advanced to allow a forward posturing of the lower jaw and balance of the TM joint and facial musculature. Development of the mid-face like these cases is expected when the palate is sufficiently widened prior to dental correction. No forward-pull head gear was used here, although we do occasionally use it in conjunction with the palatal expansion. The pre-and post-treatment models of this patient (Figs. 17 & 18) show a typical change in size and form of the palate. This case is a 31-year-old male patient with a Class II, Division 2 malocclusion, with a very narrow palate, deep bite, rabitted (reclined) central incisors and vertical range www.orthodontics.com Winter 2014 21
Journal of the American Orthodontic Society Winter 2014: Page 21