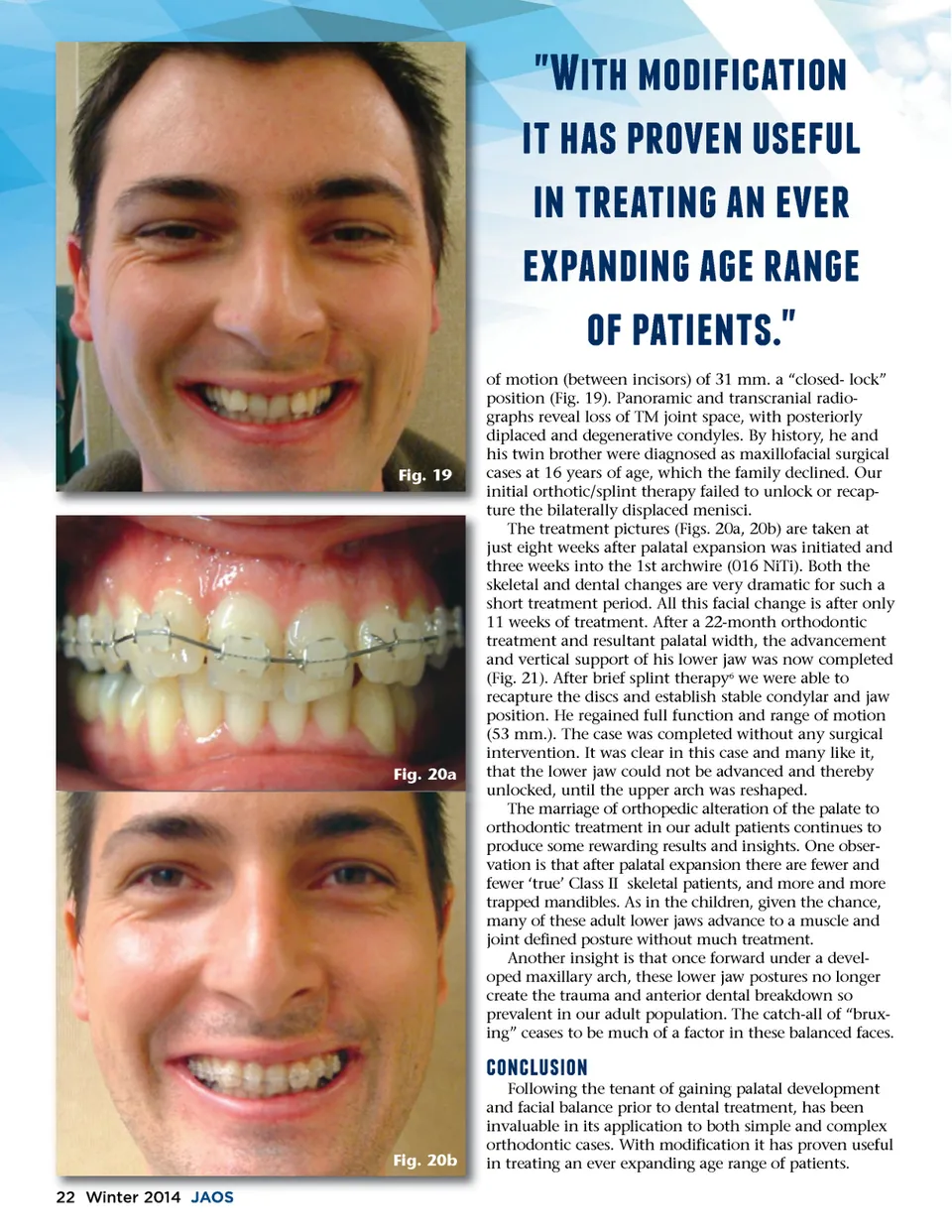
�c;45%7/)4$4(354/2 457%317#*/627 16$ , 4275*63542d;732766* 6#32)42d;73d;67*32d;6 /$7#3546251  Fig. 19 of motion (between incisors) of 31 mm. a “closed-lock” position (Fig. 19). Panoramic and transcranial radio-graphs reveal loss of TM joint space, with posteriorly diplaced and degenerative condyles. By history, he and his twin brother were diagnosed as maxillofacial surgical cases at 16 years of age, which the family declined. Our initial orthotic/splint therapy failed to unlock or recap-ture the bilaterally displaced menisci. The treatment pictures (Figs. 20a, 20b) are taken at just eight weeks after palatal expansion was initiated and three weeks into the 1st archwire (016 NiTi). Both the skeletal and dental changes are very dramatic for such a short treatment period. All this facial change is after only 11 weeks of treatment. After a 22-month orthodontic treatment and resultant palatal width, the advancement and vertical support of his lower jaw was now completed (Fig. 21). After brief splint therapy 6 we were able to recapture the discs and establish stable condylar and jaw position. He regained full function and range of motion (53 mm.). The case was completed without any surgical intervention. It was clear in this case and many like it, that the lower jaw could not be advanced and thereby unlocked, until the upper arch was reshaped. The marriage of orthopedic alteration of the palate to orthodontic treatment in our adult patients continues to produce some rewarding results and insights. One obser-vation is that after palatal expansion there are fewer and fewer ‘true’ Class II skeletal patients, and more and more trapped mandibles. As in the children, given the chance, many of these adult lower jaws advance to a muscle and joint defined posture without much treatment. Another insight is that once forward under a devel-oped maxillary arch, these lower jaw postures no longer create the trauma and anterior dental breakdown so prevalent in our adult population. The catch-all of “brux-ing” ceases to be much of a factor in these balanced faces. Fig. 20a (/2(, 14/2 Following the tenant of gaining palatal development and facial balance prior to dental treatment, has been invaluable in its application to both simple and complex orthodontic cases. With modification it has proven useful in treating an ever expanding age range of patients. Fig. 20b 22 Winter 2014 JAOS
Journal of the American Orthodontic Society Winter 2014: Page 22