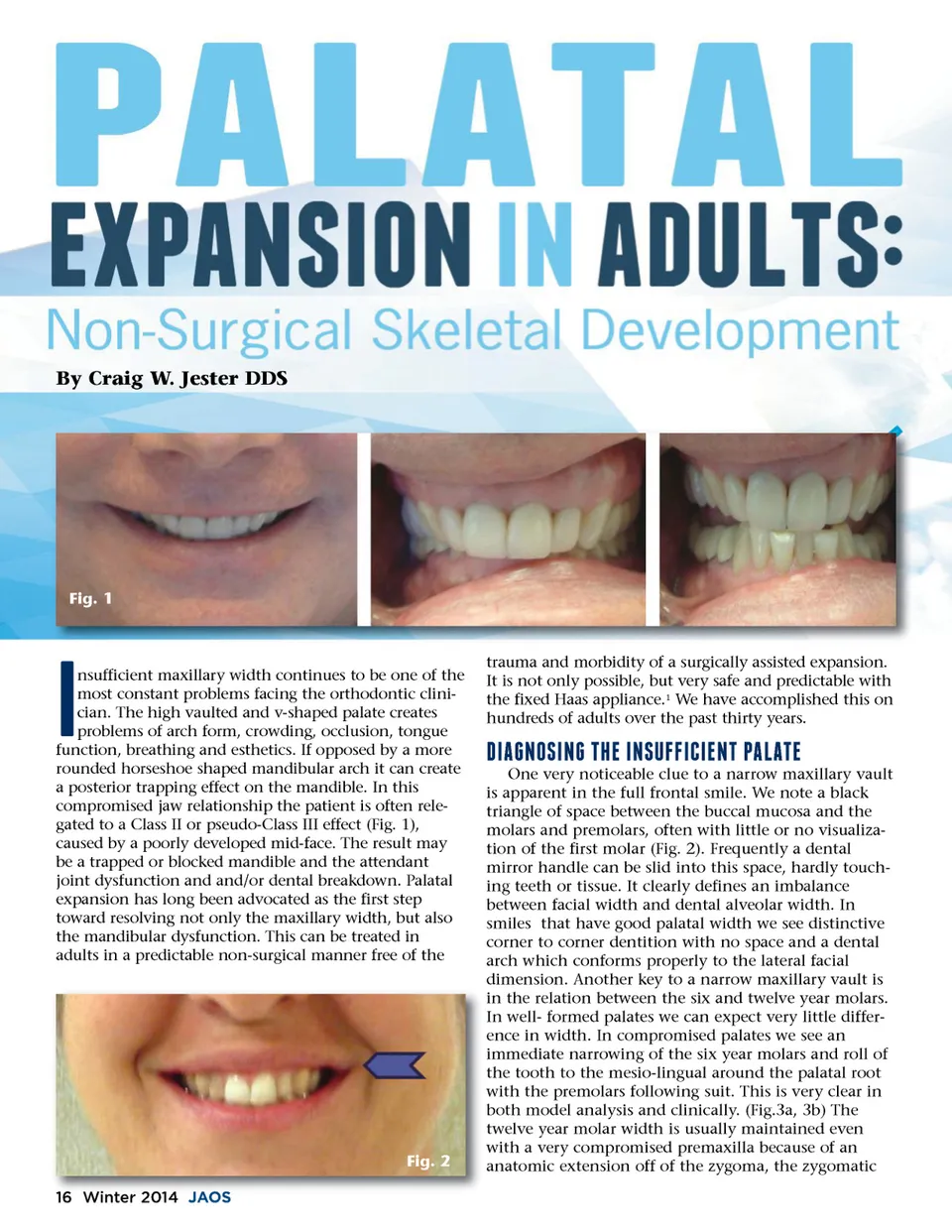
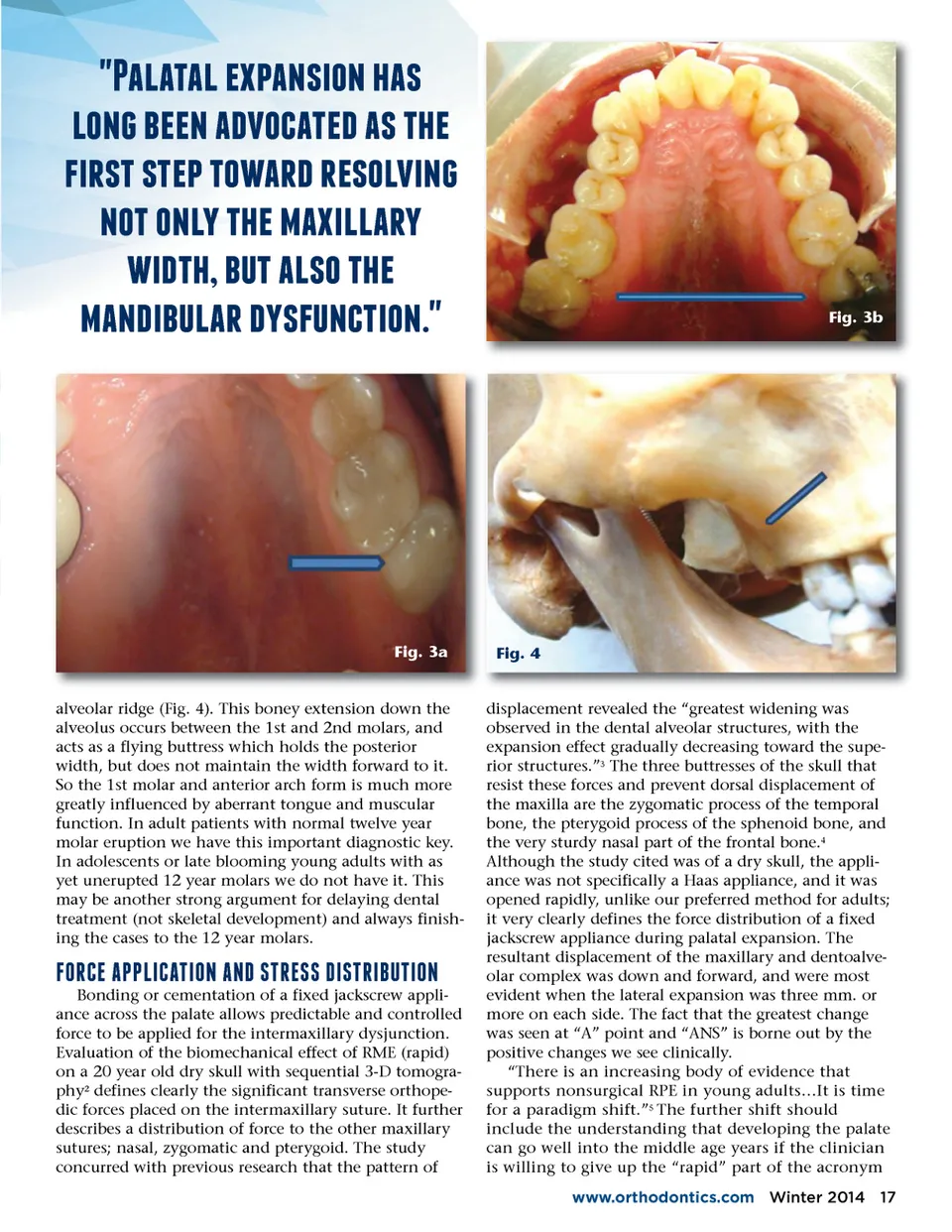
By Craig W. Jester DDS Fig. 1 nsufficient maxillary width continues to be one of the most constant problems facing the orthodontic clini-cian. The high vaulted and v-shaped palate creates problems of arch form, crowding, occlusion, tongue function, breathing and esthetics. If opposed by a more rounded horseshoe shaped mandibular arch it can create a posterior trapping effect on the mandible. In this compromised jaw relationship the patient is often rele-gated to a Class II or pseudo-Class III effect (Fig. 1), caused by a poorly developed mid-face. The result may be a trapped or blocked mandible and the attendant joint dysfunction and and/or dental breakdown. Palatal expansion has long been advocated as the first step toward resolving not only the maxillary width, but also the mandibular dysfunction. This can be treated in adults in a predictable non-surgical manner free of the -trauma and morbidity of a surgically assisted expansion. It is not only possible, but very safe and predictable with the fixed Haas appliance. 1 We have accomplished this on hundreds of adults over the past thirty years. f;-+."!-.7'07-.!c;c;-&-0.'7a;+e;+'07 One very noticeable clue to a narrow maxillary vault is apparent in the full frontal smile. We note a black triangle of space between the buccal mucosa and the molars and premolars, often with little or no visualiza-tion of the first molar (Fig. 2). Frequently a dental mirror handle can be slid into this space, hardly touch-ing teeth or tissue. It clearly defines an imbalance between facial width and dental alveolar width. In smiles that have good palatal width we see distinctive corner to corner dentition with no space and a dental arch which conforms properly to the lateral facial dimension. Another key to a narrow maxillary vault is in the relation between the six and twelve year molars. In well-formed palates we can expect very little differ-ence in width. In compromised palates we see an immediate narrowing of the six year molars and roll of the tooth to the mesio-lingual around the palatal root with the premolars following suit. This is very clear in both model analysis and clinically. (Fig.3a, 3b) The twelve year molar width is usually maintained even with a very compromised premaxilla because of an anatomic extension off of the zygoma, the zygomatic Fig. 2 16 Winter 2014 JAOS
Journal of the American Orthodontic Society Winter 2014: Page 16