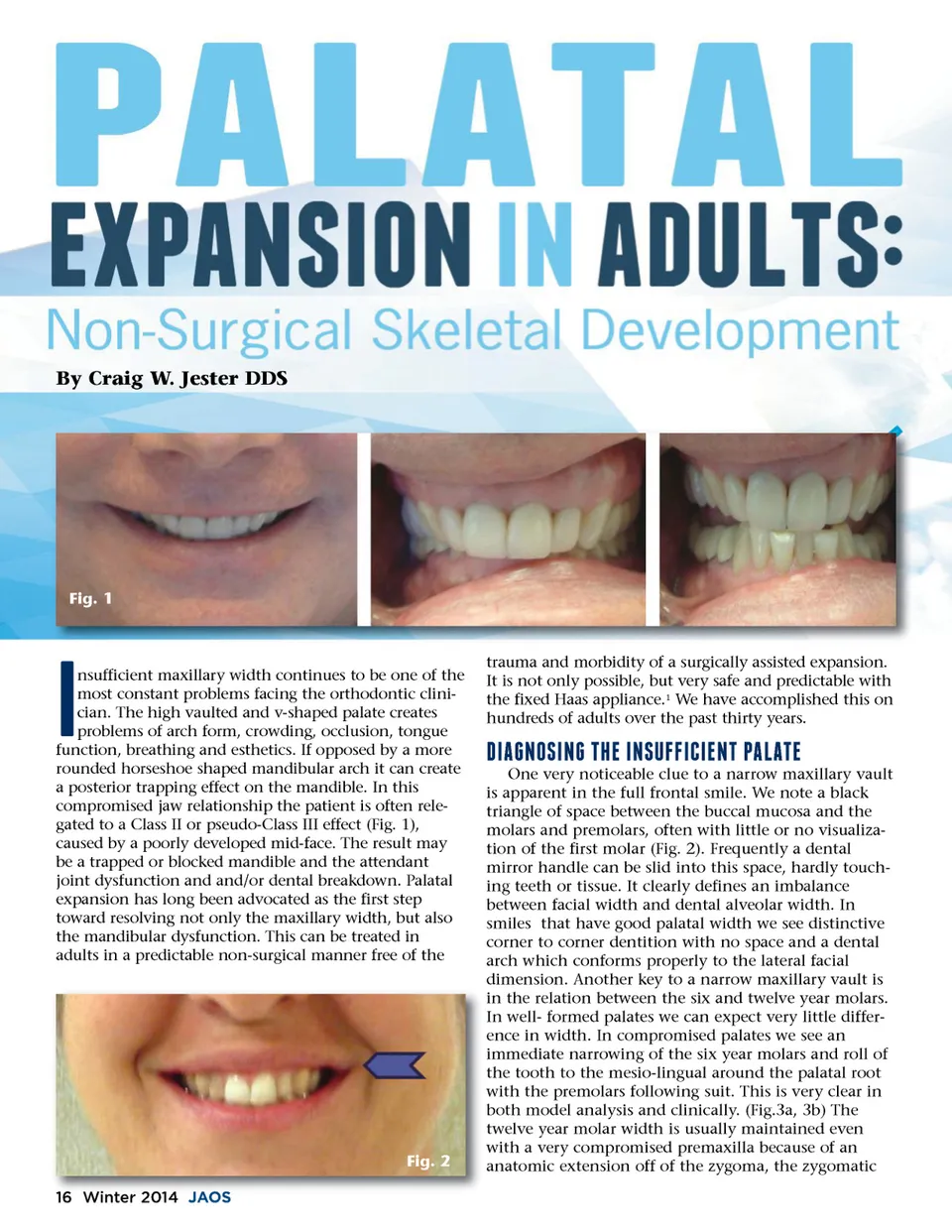
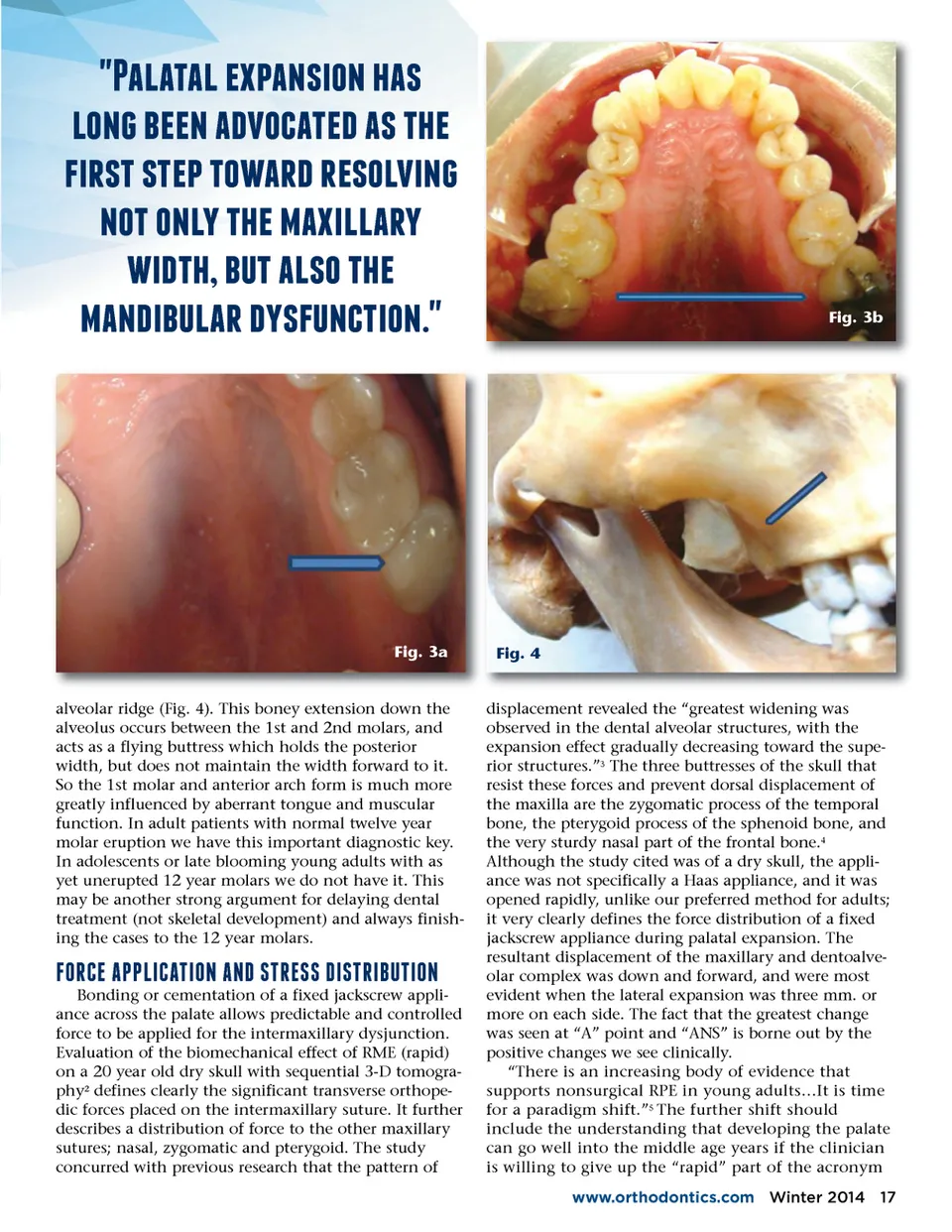
a;3,353,76#3214/27%31 ,/2d;7�f;66273)/(356)73175%6 $4*157156#75/3*)7*61/,42d; 2/57/2, 75%6734,,3* 4)5%7�f; 573,1/75%6 32)4�f; ,3*7) 1$ 2(54/2  Fig. 3b Fig. 3a Fig. 4 alveolar ridge (Fig. 4). This boney extension down the alveolus occurs between the 1st and 2nd molars, and acts as a flying buttress which holds the posterior width, but does not maintain the width forward to it. So the 1st molar and anterior arch form is much more greatly influenced by aberrant tongue and muscular function. In adult patients with normal twelve year molar eruption we have this important diagnostic key. In adolescents or late blooming young adults with as yet unerupted 12 year molars we do not have it. This may be another strong argument for delaying dental treatment (not skeletal development) and always finish-ing the cases to the 12 year molars. c;"b;&07+a;a;e;-&+'-".7+.f;7!'b;0!!7f;-!'b;-�d;'-".7 Bonding or cementation of a fixed jackscrew appli-ance across the palate allows predictable and controlled force to be applied for the intermaxillary dysjunction. Evaluation of the biomechanical effect of RME (rapid) on a 20 year old dry skull with sequential 3-D tomogra-phy 2 defines clearly the significant transverse orthope-dic forces placed on the intermaxillary suture. It further describes a distribution of force to the other maxillary sutures; nasal, zygomatic and pterygoid. The study concurred with previous research that the pattern of displacement revealed the “greatest widening was observed in the dental alveolar structures, with the expansion effect gradually decreasing toward the supe-rior structures.” 3 The three buttresses of the skull that resist these forces and prevent dorsal displacement of the maxilla are the zygomatic process of the temporal bone, the pterygoid process of the sphenoid bone, and the very sturdy nasal part of the frontal bone. 4 Although the study cited was of a dry skull, the appli-ance was not specifically a Haas appliance, and it was opened rapidly, unlike our preferred method for adults; it very clearly defines the force distribution of a fixed jackscrew appliance during palatal expansion. The resultant displacement of the maxillary and dentoalve-olar complex was down and forward, and were most evident when the lateral expansion was three mm. or more on each side. The fact that the greatest change was seen at “A” point and “ANS” is borne out by the positive changes we see clinically. “There is an increasing body of evidence that supports nonsurgical RPE in young adults…It is time for a paradigm shift.” 5 The further shift should include the understanding that developing the palate can go well into the middle age years if the clinician is willing to give up the “rapid” part of the acronym www.orthodontics.com Winter 2014 17
Journal of the American Orthodontic Society Winter 2014: Page 17