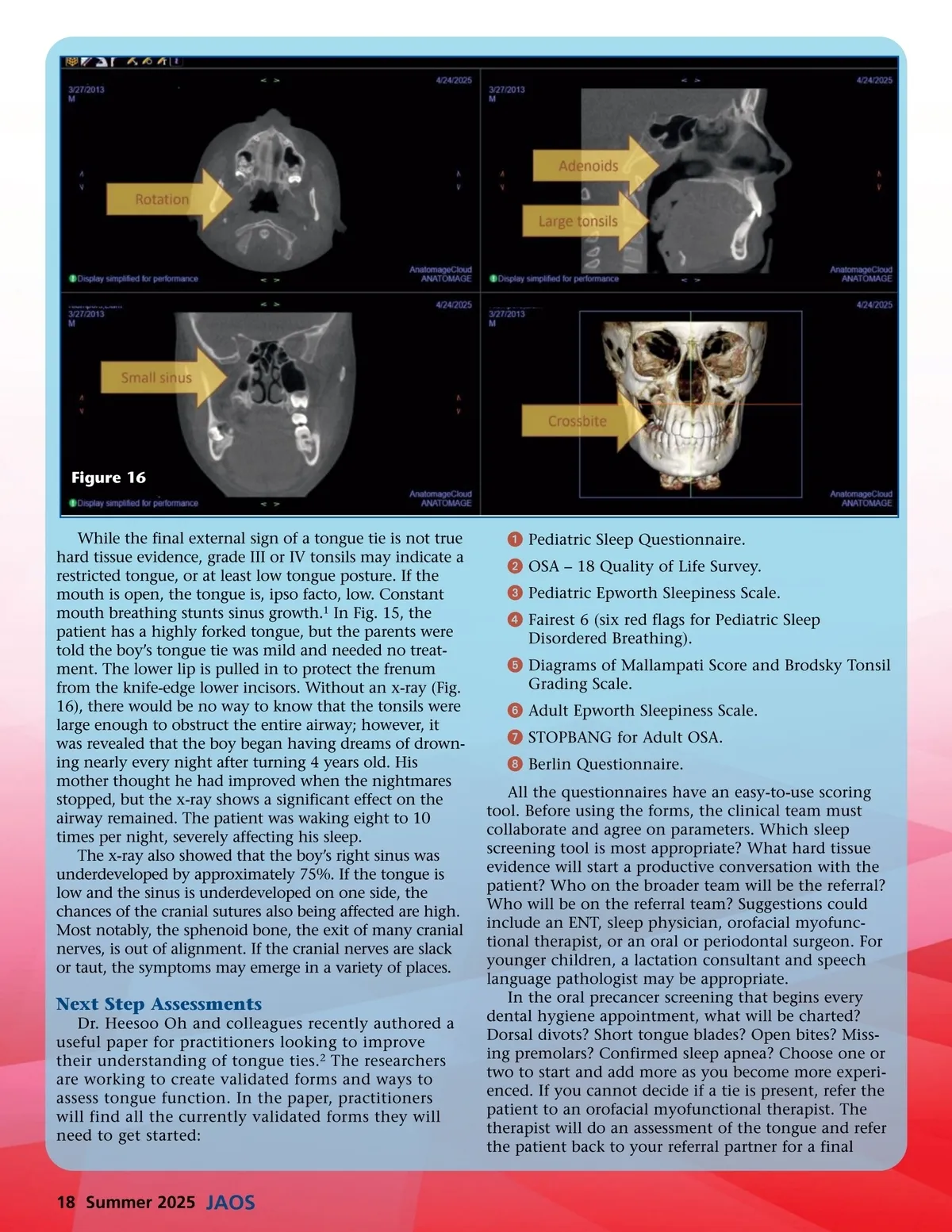
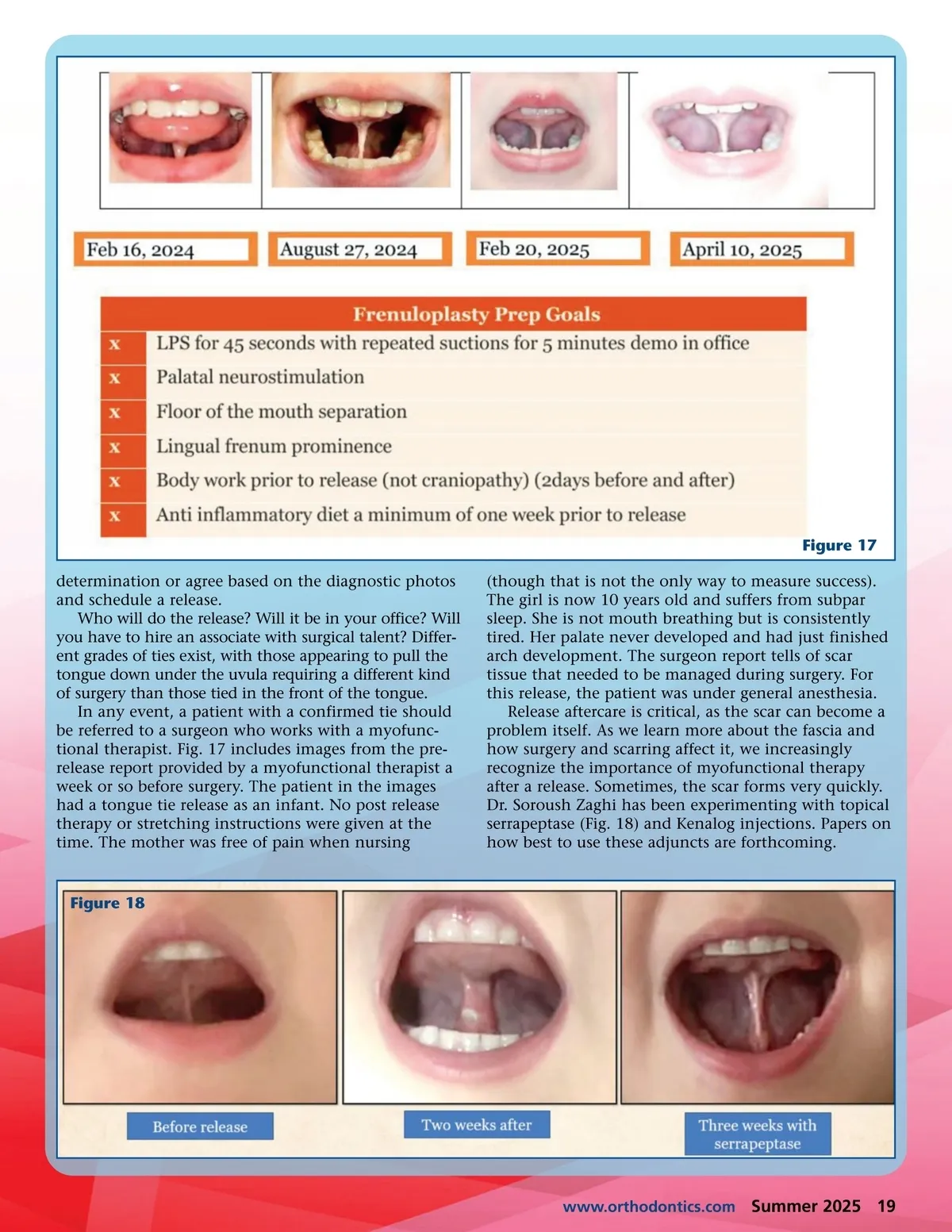
Figure 17 determination or agree based on the diagnostic photos and schedule a release. Who will do the release? Will it be in your office? Will you have to hire an associate with surgical talent? Differ-ent grades of ties exist, with those appearing to pull the tongue down under the uvula requiring a different kind of surgery than those tied in the front of the tongue. In any event, a patient with a confirmed tie should be referred to a surgeon who works with a myofunc-tional therapist. Fig. 17 includes images from the pre-release report provided by a myofunctional therapist a week or so before surgery. The patient in the images had a tongue tie release as an infant. No post release therapy or stretching instructions were given at the time. The mother was free of pain when nursing (though that is not the only way to measure success). The girl is now 10 years old and suffers from subpar sleep. She is not mouth breathing but is consistently tired. Her palate never developed and had just finished arch development. The surgeon report tells of scar tissue that needed to be managed during surgery. For this release, the patient was under general anesthesia. Release aftercare is critical, as the scar can become a problem itself. As we learn more about the fascia and how surgery and scarring affect it, we increasingly recognize the importance of myofunctional therapy after a release. Sometimes, the scar forms very quickly. Dr. Soroush Zaghi has been experimenting with topical serrapeptase (Fig. 18) and Kenalog injections. Papers on how best to use these adjuncts are forthcoming. Figure 18 www.orthodontics.com Summer 2025 19
Journal of the American Orthodontic Society Summer 2025: Page 19