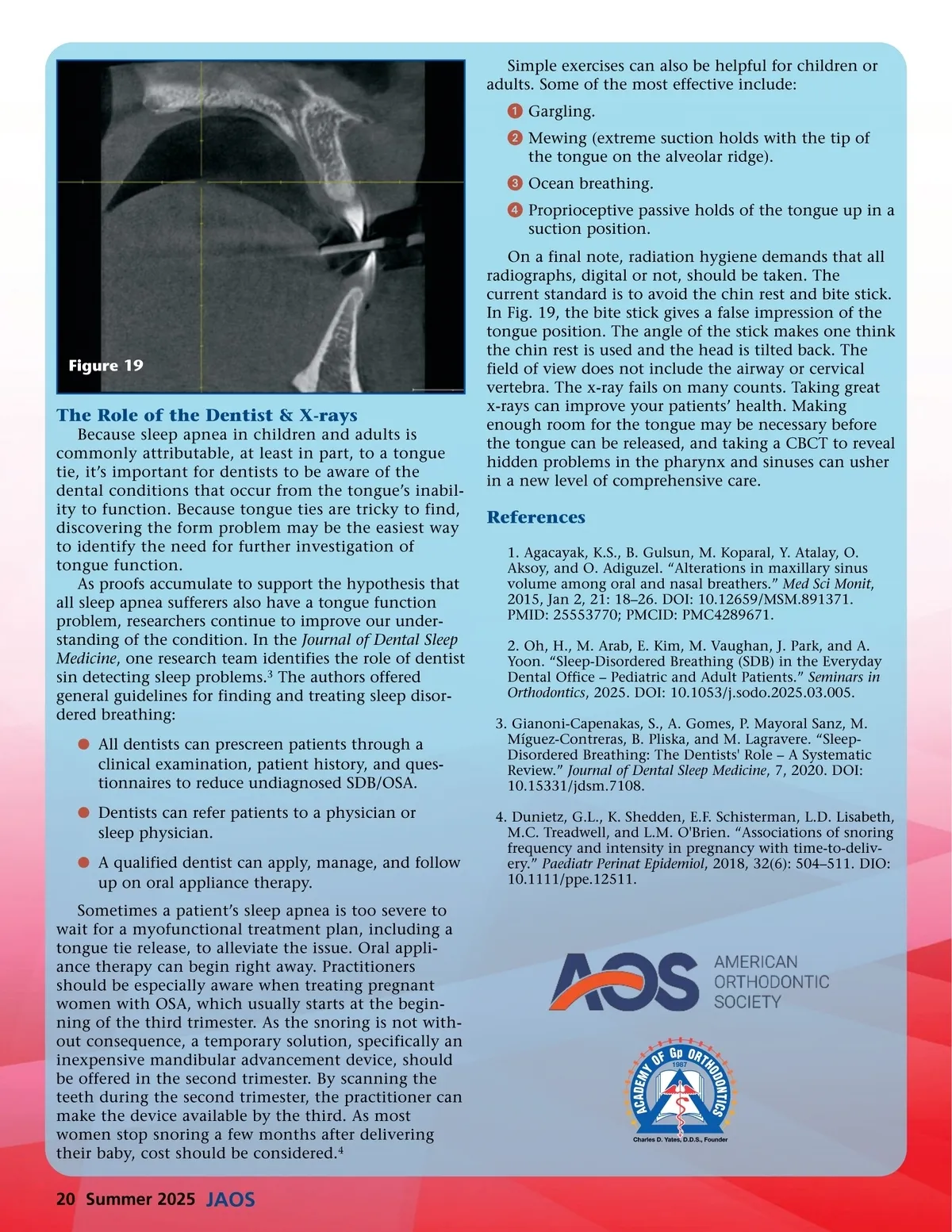
Simple exercises can also be helpful for children or adults. Some of the most effective include: ᕡ Gargling. ᕢ Mewing (extreme suction holds with the tip of the tongue on the alveolar ridge). ᕣ Ocean breathing. ᕤ Proprioceptive passive holds of the tongue up in a suction position. On a final note, radiation hygiene demands that all radiographs, digital or not, should be taken. The current standard is to avoid the chin rest and bite stick. In Fig. 19, the bite stick gives a false impression of the tongue position. The angle of the stick makes one think the chin rest is used and the head is tilted back. The field of view does not include the airway or cervical vertebra. The x-ray fails on many counts. Taking great x-rays can improve your patients’ health. Making enough room for the tongue may be necessary before the tongue can be released, and taking a CBCT to reveal hidden problems in the pharynx and sinuses can usher in a new level of comprehensive care. Figure 19 The Role of the Dentist & X-rays Because sleep apnea in children and adults is commonly attributable, at least in part, to a tongue tie, it’s important for dentists to be aware of the dental conditions that occur from the tongue’s inabil-ity to function. Because tongue ties are tricky to find, discovering the form problem may be the easiest way to identify the need for further investigation of tongue function. As proofs accumulate to support the hypothesis that all sleep apnea sufferers also have a tongue function problem, researchers continue to improve our under-standing of the condition. In the Journal of Dental Sleep Medicine , one research team identifies the role of dentist sin detecting sleep problems. 3 The authors offered general guidelines for finding and treating sleep disor-dered breathing: b All dentists can prescreen patients through a clinical examination, patient history, and ques-tionnaires to reduce undiagnosed SDB/OSA. b Dentists can refer patients to a physician or sleep physician. b A qualified dentist can apply, manage, and follow up on oral appliance therapy. Sometimes a patient’s sleep apnea is too severe to wait for a myofunctional treatment plan, including a tongue tie release, to alleviate the issue. Oral appli-ance therapy can begin right away. Practitioners should be especially aware when treating pregnant women with OSA, which usually starts at the begin-ning of the third trimester. As the snoring is not with-out consequence, a temporary solution, specifically an inexpensive mandibular advancement device, should be offered in the second trimester. By scanning the teeth during the second trimester, the practitioner can make the device available by the third. As most women stop snoring a few months after delivering their baby, cost should be considered. 4 References 1. Agacayak, K.S., B. Gulsun, M. Koparal, Y. Atalay, O. Aksoy, and O. Adiguzel. “Alterations in maxillary sinus volume among oral and nasal breathers.” Med Sci Monit , 2015, Jan 2, 21: 18–26. DOI: 10.12659/MSM.891371. PMID: 25553770; PMCID: PMC4289671. 2. Oh, H., M. Arab, E. Kim, M. Vaughan, J. Park, and A. Yoon. “Sleep-Disordered Breathing (SDB) in the Everyday Dental Office – Pediatric and Adult Patients.” Seminars in Orthodontics , 2025. DOI: 10.1053/j.sodo.2025.03.005. 3. Gianoni-Capenakas, S., A. Gomes, P. Mayoral Sanz, M. Míguez-Contreras, B. Pliska, and M. Lagravere. “Sleep-Disordered Breathing: The Dentists' Role – A Systematic Review.” Journal of Dental Sleep Medicine , 7, 2020. DOI: 10.15331/jdsm.7108. 4. Dunietz, G.L., K. Shedden, E.F. Schisterman, L.D. Lisabeth, M.C. Treadwell, and L.M. O'Brien. “Associations of snoring frequency and intensity in pregnancy with time-to-deliv-ery.” Paediatr Perinat Epidemiol , 2018, 32(6): 504–511. DIO: 10.1111/ppe.12511. 20 Summer 2025 JAOS
Journal of the American Orthodontic Society Summer 2025: Page 20