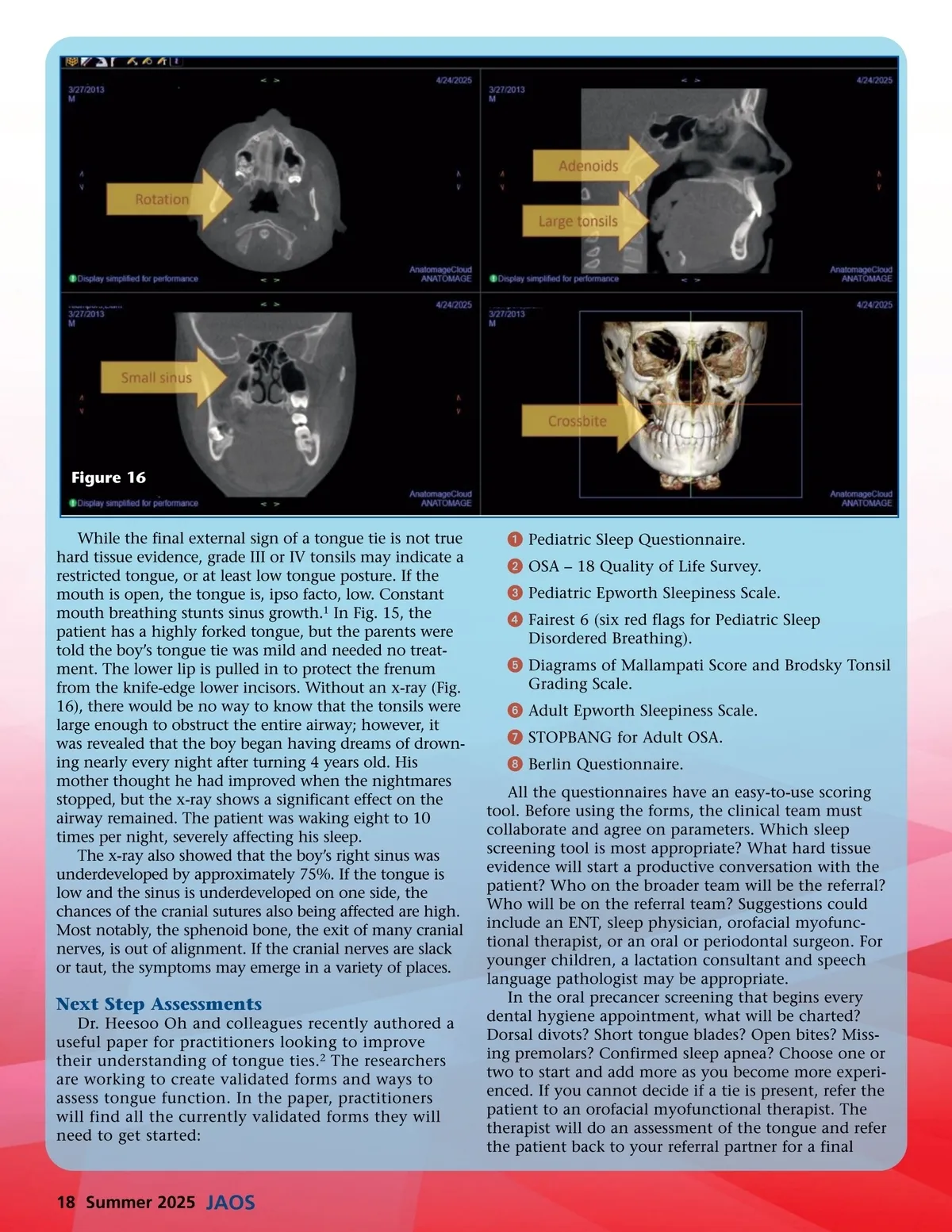
Figure 16 While the final external sign of a tongue tie is not true hard tissue evidence, grade III or IV tonsils may indicate a restricted tongue, or at least low tongue posture. If the mouth is open, the tongue is, ipso facto, low. Constant mouth breathing stunts sinus growth. 1 In Fig. 15, the patient has a highly forked tongue, but the parents were told the boy’s tongue tie was mild and needed no treat-ment. The lower lip is pulled in to protect the frenum from the knife-edge lower incisors. Without an x-ray (Fig. 16), there would be no way to know that the tonsils were large enough to obstruct the entire airway; however, it was revealed that the boy began having dreams of drown-ing nearly every night after turning 4 years old. His mother thought he had improved when the nightmares stopped, but the x-ray shows a significant effect on the airway remained. The patient was waking eight to 10 times per night, severely affecting his sleep. The x-ray also showed that the boy’s right sinus was underdeveloped by approximately 75%. If the tongue is low and the sinus is underdeveloped on one side, the chances of the cranial sutures also being affected are high. Most notably, the sphenoid bone, the exit of many cranial nerves, is out of alignment. If the cranial nerves are slack or taut, the symptoms may emerge in a variety of places. ᕡ Pediatric Sleep Questionnaire. ᕢ OSA – 18 Quality of Life Survey. ᕣ Pediatric Epworth Sleepiness Scale. ᕤ Fairest 6 (six red flags for Pediatric Sleep Disordered Breathing). ᕥ Diagrams of Mallampati Score and Brodsky Tonsil Grading Scale. ᕦ Adult Epworth Sleepiness Scale. ᕧ STOPBANG for Adult OSA. ᕨ Berlin Questionnaire. All the questionnaires have an easy-to-use scoring tool. Before using the forms, the clinical team must collaborate and agree on parameters. Which sleep screening tool is most appropriate? What hard tissue evidence will start a productive conversation with the patient? Who on the broader team will be the referral? Who will be on the referral team? Suggestions could include an ENT, sleep physician, orofacial myofunc-tional therapist, or an oral or periodontal surgeon. For younger children, a lactation consultant and speech language pathologist may be appropriate. In the oral precancer screening that begins every dental hygiene appointment, what will be charted? Dorsal divots? Short tongue blades? Open bites? Miss-ing premolars? Confirmed sleep apnea? Choose one or two to start and add more as you become more experi-enced. If you cannot decide if a tie is present, refer the patient to an orofacial myofunctional therapist. The therapist will do an assessment of the tongue and refer the patient back to your referral partner for a final Next Step Assessments Dr. Heesoo Oh and colleagues recently authored a useful paper for practitioners looking to improve their understanding of tongue ties. 2 The researchers are working to create validated forms and ways to assess tongue function. In the paper, practitioners will find all the currently validated forms they will need to get started: 18 Summer 2025 JAOS
Journal of the American Orthodontic Society Summer 2025: Page 18