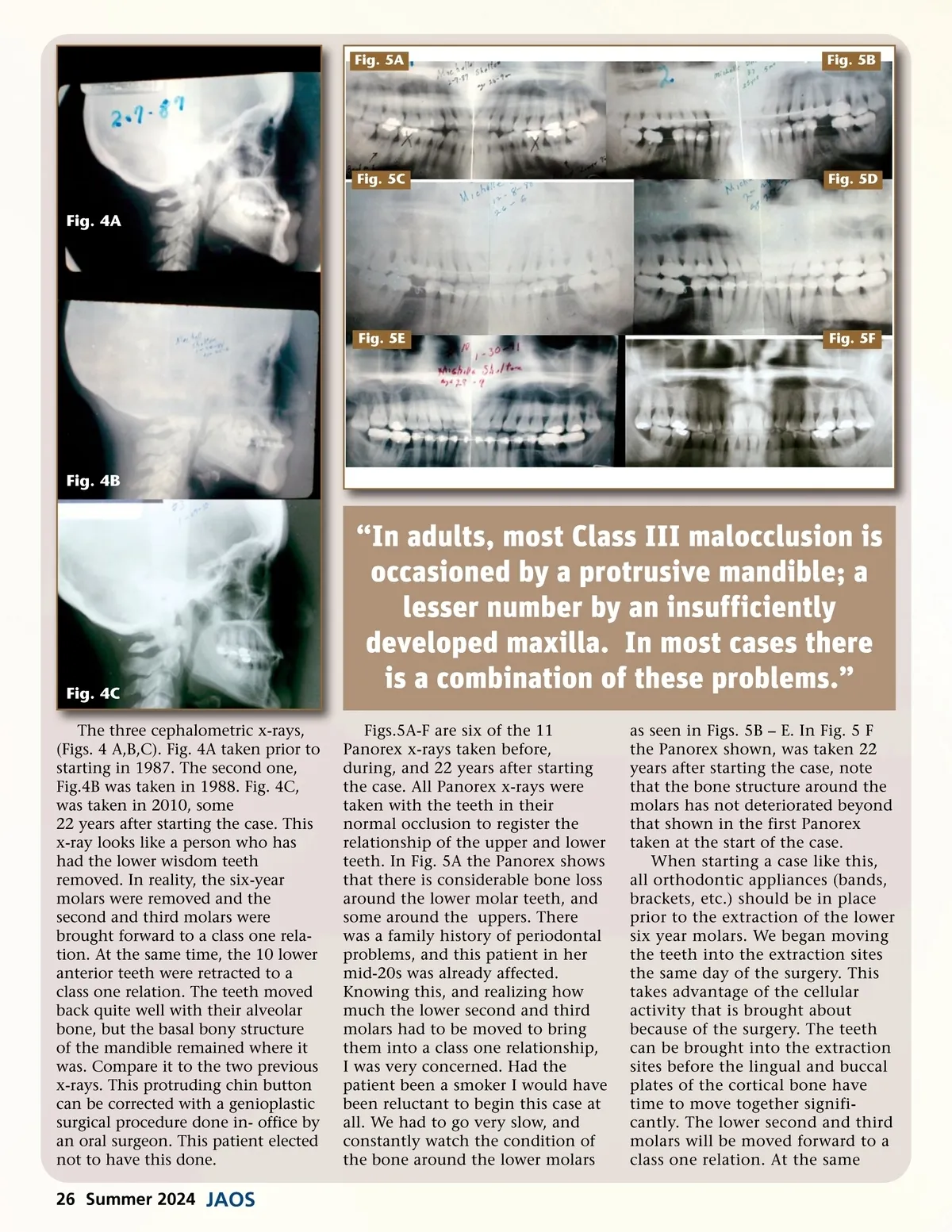
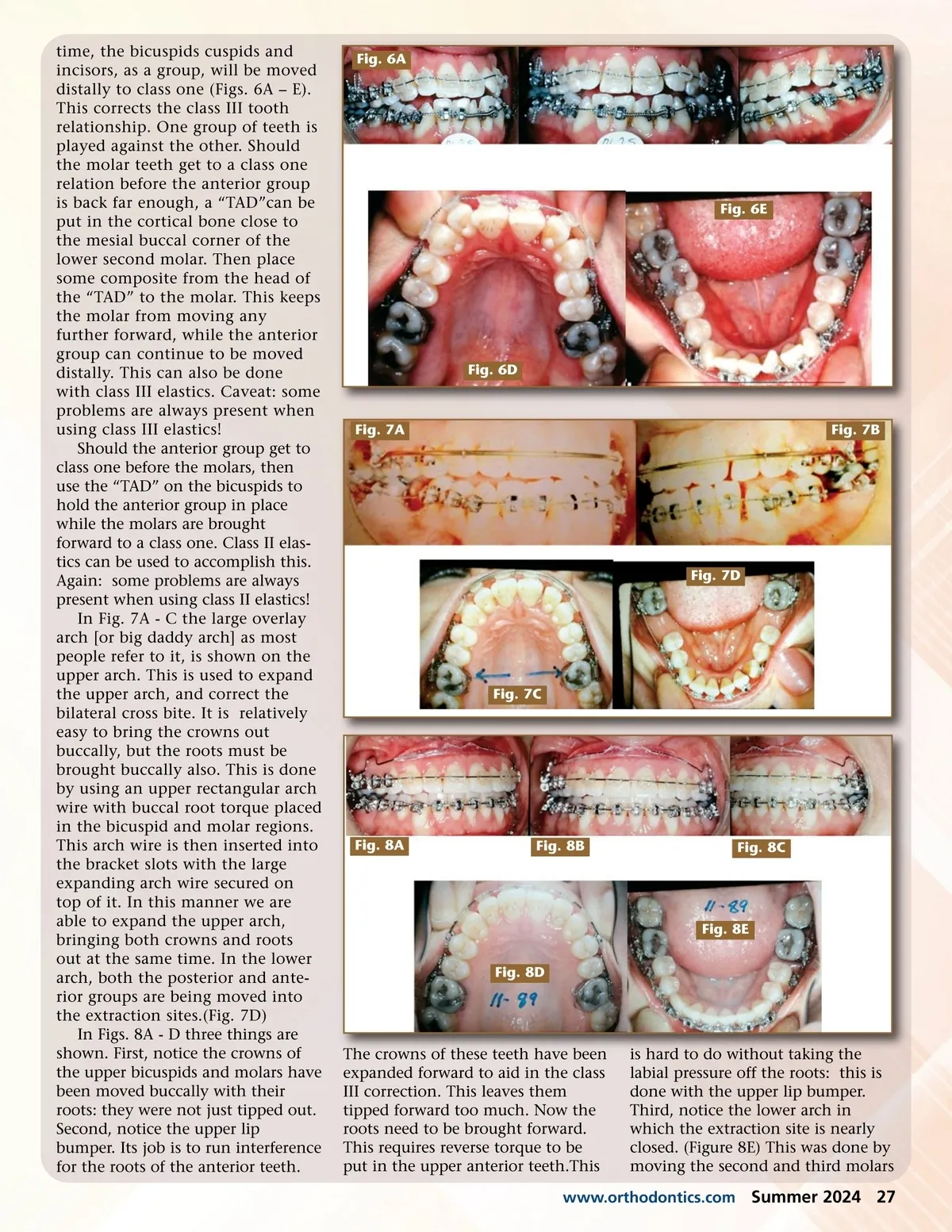
Fig. 5A Fig. 5B Fig. 5C Fig. 5D Fig. 4A Fig. 5E Fig. 5F Fig. 4B Fig. 4C The three cephalometric x-rays, (Figs. 4 A,B,C). Fig. 4A taken prior to starting in 1987. The second one, Fig.4B was taken in 1988. Fig. 4C, was taken in 2010, some 22 years after starting the case. This x-ray looks like a person who has had the lower wisdom teeth removed. In reality, the six-year molars were removed and the second and third molars were brought forward to a class one rela-tion. At the same time, the 10 lower anterior teeth were retracted to a class one relation. The teeth moved back quite well with their alveolar bone, but the basal bony structure of the mandible remained where it was. Compare it to the two previous x-rays. This protruding chin button can be corrected with a genioplastic surgical procedure done in-office by an oral surgeon. This patient elected not to have this done. “In adults, most Class III malocclusion is occasioned by a protrusive mandible; a lesser number by an insufficiently developed maxilla. In most cases there is a combination of these problems.” Figs.5A-F are six of the 11 Panorex x-rays taken before, during, and 22 years after starting the case. All Panorex x-rays were taken with the teeth in their normal occlusion to register the relationship of the upper and lower teeth. In Fig. 5A the Panorex shows that there is considerable bone loss around the lower molar teeth, and some around the uppers. There was a family history of periodontal problems, and this patient in her mid-20s was already affected. Knowing this, and realizing how much the lower second and third molars had to be moved to bring them into a class one relationship, I was very concerned. Had the patient been a smoker I would have been reluctant to begin this case at all. We had to go very slow, and constantly watch the condition of the bone around the lower molars as seen in Figs. 5B – E. In Fig. 5 F the Panorex shown, was taken 22 years after starting the case, note that the bone structure around the molars has not deteriorated beyond that shown in the first Panorex taken at the start of the case. When starting a case like this, all orthodontic appliances (bands, brackets, etc.) should be in place prior to the extraction of the lower six year molars. We began moving the teeth into the extraction sites the same day of the surgery. This takes advantage of the cellular activity that is brought about because of the surgery. The teeth can be brought into the extraction sites before the lingual and buccal plates of the cortical bone have time to move together signifi-cantly. The lower second and third molars will be moved forward to a class one relation. At the same 26 Summer 2024 JAOS
Journal of the American Orthodontic Society Summer 2024: Page 26