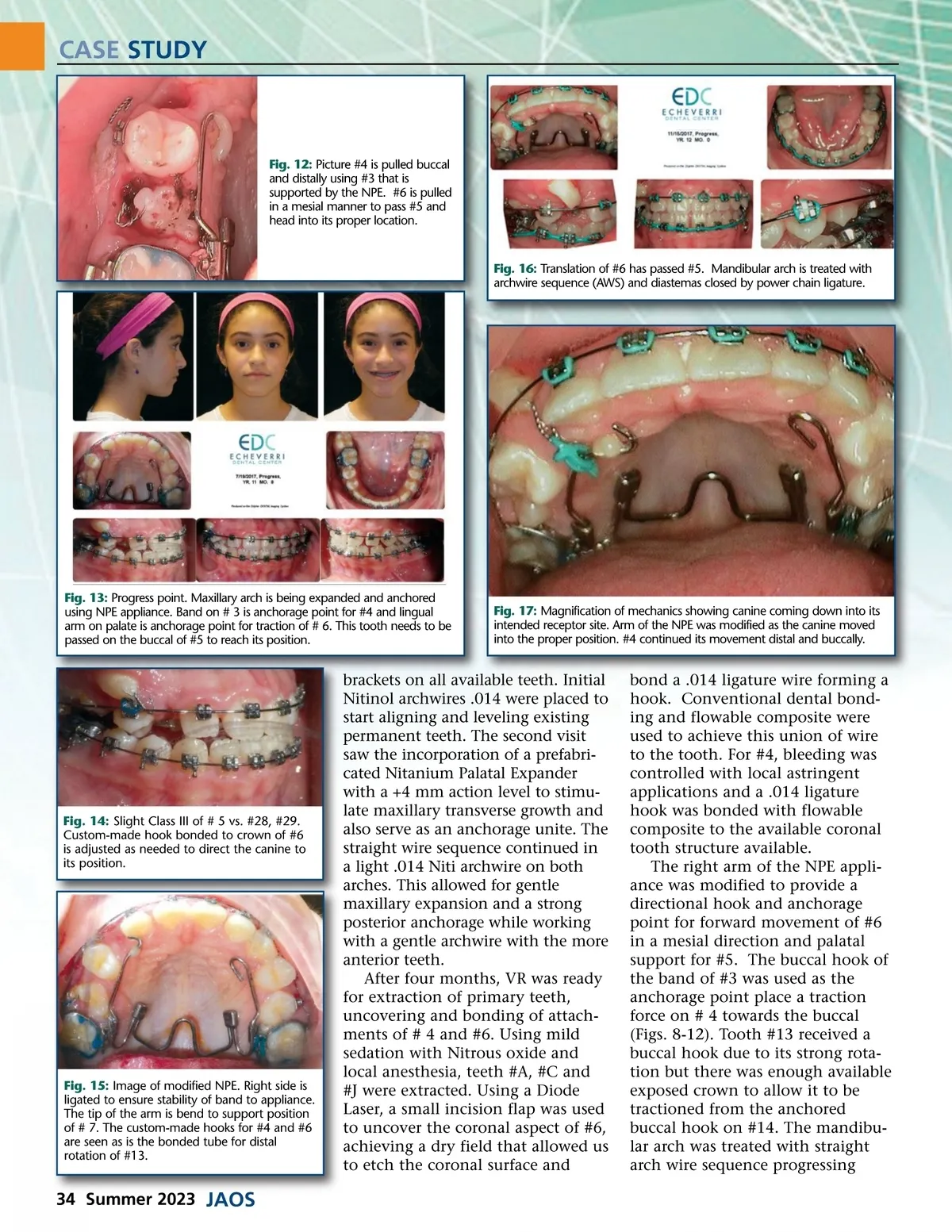
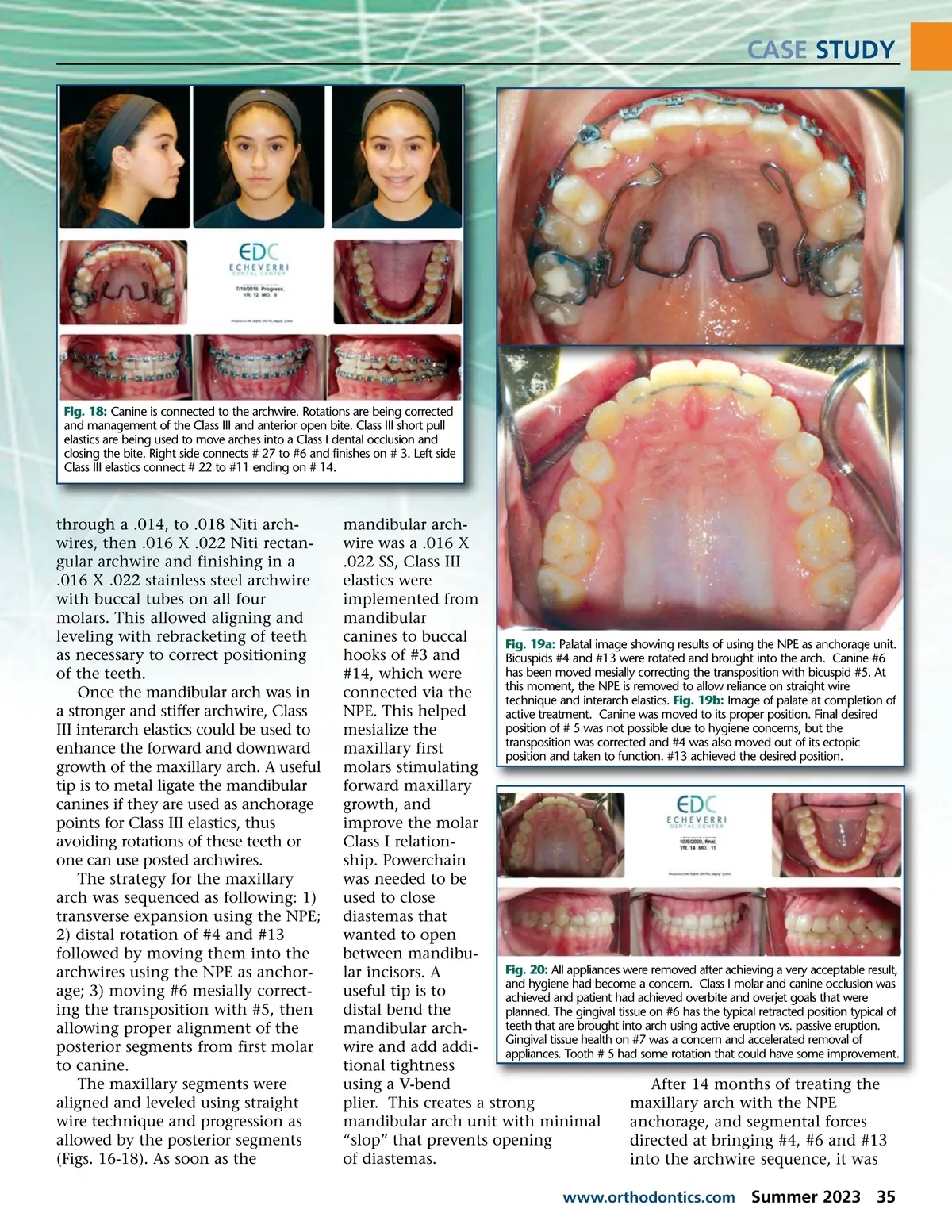
CASE STUDY Fig. 18: Canine is connected to the archwire. Rotations are being corrected and management of the Class III and anterior open bite. Class III short pull elastics are being used to move arches into a Class I dental occlusion and closing the bite. Right side connects # 27 to #6 and finishes on # 3. Left side Class III elastics connect # 22 to #11 ending on # 14. through a .014, to .018 Niti arch-wires, then .016 X .022 Niti rectan-gular archwire and finishing in a .016 X .022 stainless steel archwire with buccal tubes on all four molars. This allowed aligning and leveling with rebracketing of teeth as necessary to correct positioning of the teeth. Once the mandibular arch was in a stronger and stiffer archwire, Class III interarch elastics could be used to enhance the forward and downward growth of the maxillary arch. A useful tip is to metal ligate the mandibular canines if they are used as anchorage points for Class III elastics, thus avoiding rotations of these teeth or one can use posted archwires. The strategy for the maxillary arch was sequenced as following: 1) transverse expansion using the NPE; 2) distal rotation of #4 and #13 followed by moving them into the archwires using the NPE as anchor-age; 3) moving #6 mesially correct-ing the transposition with #5, then allowing proper alignment of the posterior segments from first molar to canine. The maxillary segments were aligned and leveled using straight wire technique and progression as allowed by the posterior segments (Figs. 16-18). As soon as the mandibular arch-wire was a .016 X .022 SS, Class III elastics were implemented from mandibular canines to buccal Fig. 19a: Palatal image showing results of using the NPE as anchorage unit. hooks of #3 and Bicuspids #4 and #13 were rotated and brought into the arch. Canine #6 has been moved mesially correcting the transposition with bicuspid #5. At #14, which were this moment, the NPE is removed to allow reliance on straight wire connected via the technique and interarch elastics. Fig. 19b: Image of palate at completion of NPE. This helped active treatment. Canine was moved to its proper position. Final desired position of # 5 was not possible due to hygiene concerns, but the mesialize the transposition was corrected and #4 was also moved out of its ectopic maxillary first position and taken to function. #13 achieved the desired position. molars stimulating forward maxillary growth, and improve the molar Class I relation-ship. Powerchain was needed to be used to close diastemas that wanted to open between mandibu-Fig. 20: All appliances were removed after achieving a very acceptable result, lar incisors. A and hygiene had become a concern. Class I molar and canine occlusion was useful tip is to achieved and patient had achieved overbite and overjet goals that were distal bend the planned. The gingival tissue on #6 has the typical retracted position typical of teeth that are brought into arch using active eruption vs. passive eruption. mandibular arch-Gingival tissue health on #7 was a concern and accelerated removal of wire and add addi-appliances. Tooth # 5 had some rotation that could have some improvement. tional tightness using a V-bend After 14 months of treating the plier. This creates a strong maxillary arch with the NPE mandibular arch unit with minimal anchorage, and segmental forces “slop” that prevents opening directed at bringing #4, #6 and #13 of diastemas. into the archwire sequence, it was www.orthodontics.com Summer 2023 35
Journal of the American Orthodontic Society Summer 2023: Page 35