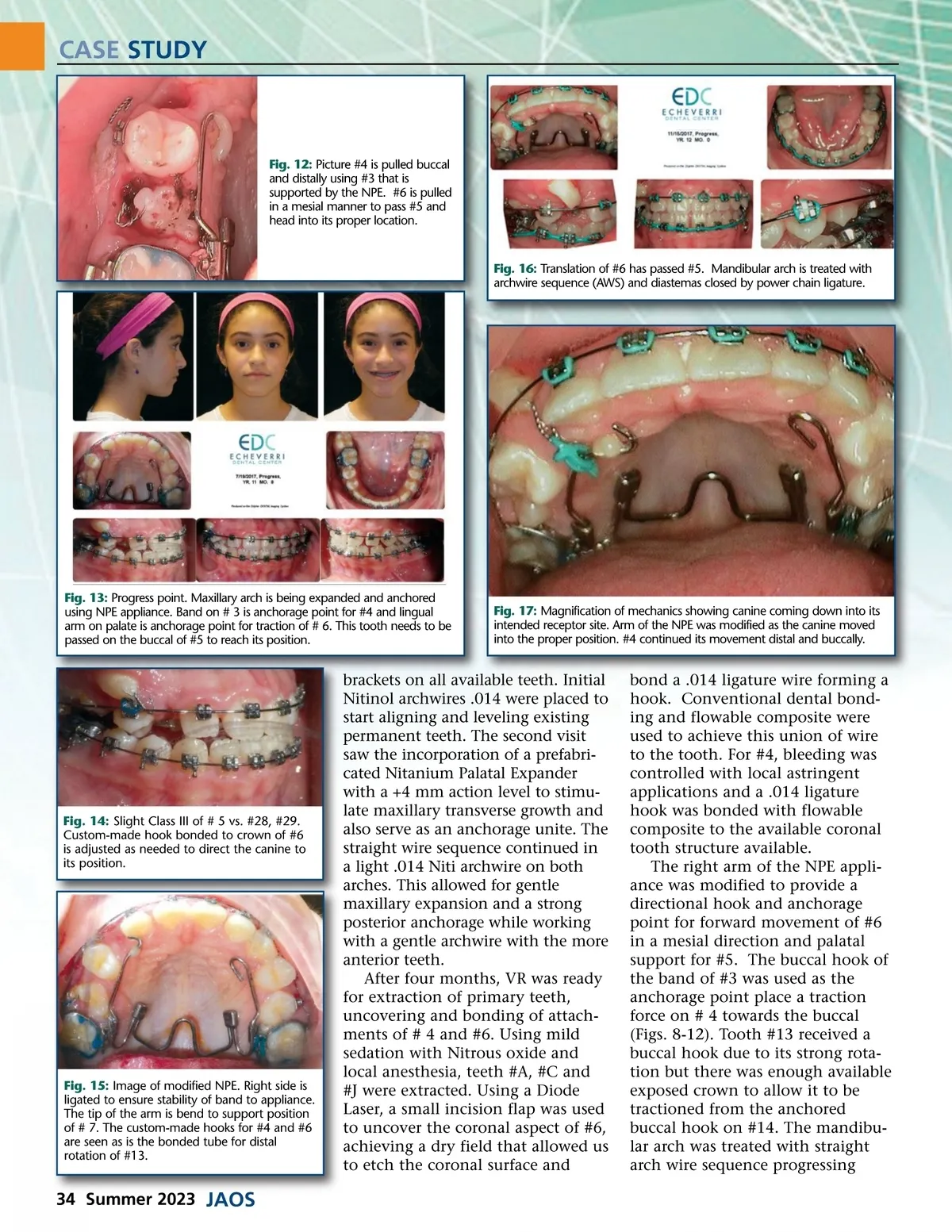
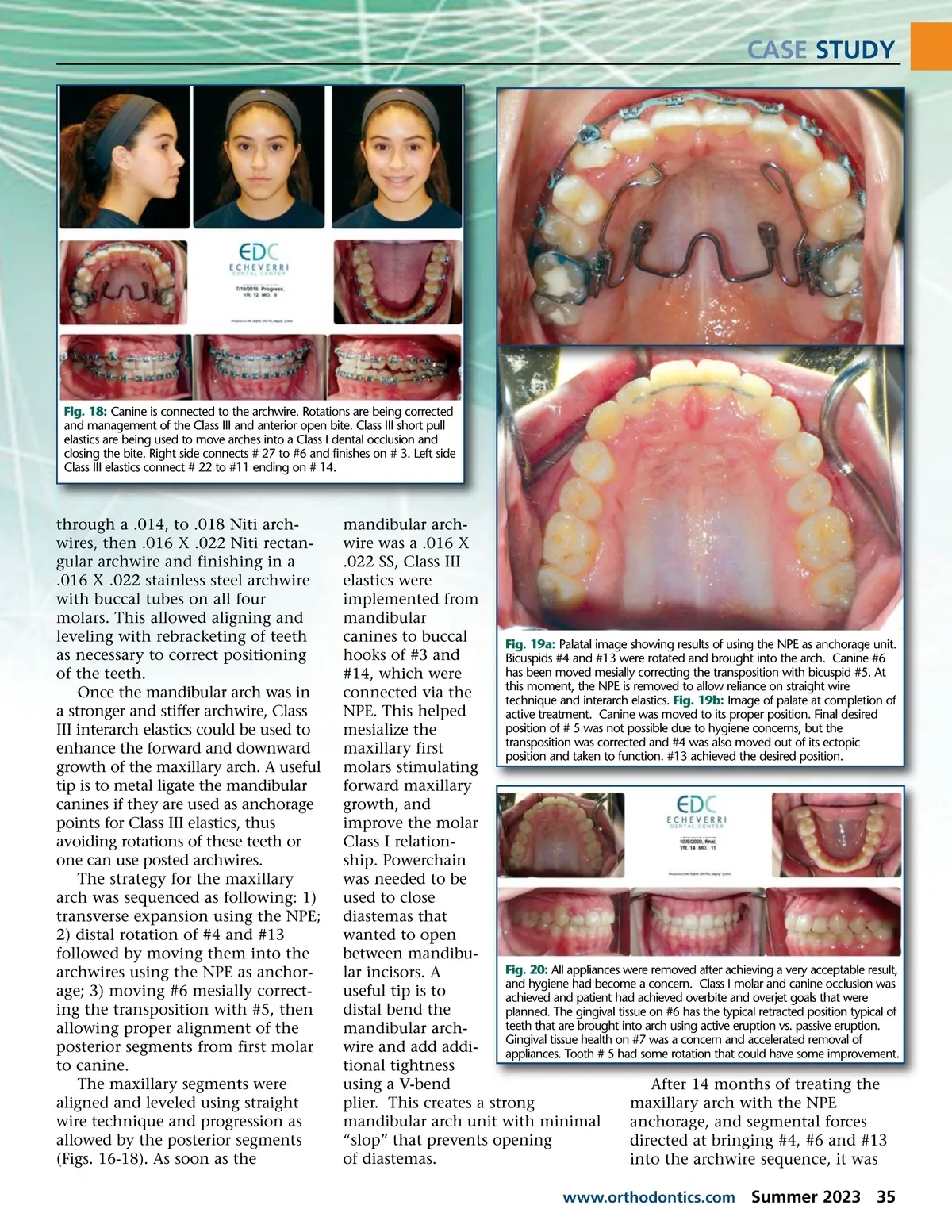
CASE STUDY Fig. 12: Picture #4 is pulled buccal and distally using #3 that is supported by the NPE. #6 is pulled in a mesial manner to pass #5 and head into its proper location. Fig. 16: Translation of #6 has passed #5. Mandibular arch is treated with archwire sequence (AWS) and diastemas closed by power chain ligature. Fig. 13: Progress point. Maxillary arch is being expanded and anchored using NPE appliance. Band on # 3 is anchorage point for #4 and lingual arm on palate is anchorage point for traction of # 6. This tooth needs to be passed on the buccal of #5 to reach its position. Fig. 17: Magnification of mechanics showing canine coming down into its intended receptor site. Arm of the NPE was modified as the canine moved into the proper position. #4 continued its movement distal and buccally. Fig. 14: Slight Class III of # 5 vs. #28, #29. Custom-made hook bonded to crown of #6 is adjusted as needed to direct the canine to its position. Fig. 15: Image of modified NPE. Right side is ligated to ensure stability of band to appliance. The tip of the arm is bend to support position of # 7. The custom-made hooks for #4 and #6 are seen as is the bonded tube for distal rotation of #13. brackets on all available teeth. Initial Nitinol archwires .014 were placed to start aligning and leveling existing permanent teeth. The second visit saw the incorporation of a prefabri-cated Nitanium Palatal Expander with a +4 mm action level to stimu-late maxillary transverse growth and also serve as an anchorage unite. The straight wire sequence continued in a light .014 Niti archwire on both arches. This allowed for gentle maxillary expansion and a strong posterior anchorage while working with a gentle archwire with the more anterior teeth. After four months, VR was ready for extraction of primary teeth, uncovering and bonding of attach-ments of # 4 and #6. Using mild sedation with Nitrous oxide and local anesthesia, teeth #A, #C and #J were extracted. Using a Diode Laser, a small incision flap was used to uncover the coronal aspect of #6, achieving a dry field that allowed us to etch the coronal surface and bond a .014 ligature wire forming a hook. Conventional dental bond-ing and flowable composite were used to achieve this union of wire to the tooth. For #4, bleeding was controlled with local astringent applications and a .014 ligature hook was bonded with flowable composite to the available coronal tooth structure available. The right arm of the NPE appli-ance was modified to provide a directional hook and anchorage point for forward movement of #6 in a mesial direction and palatal support for #5. The buccal hook of the band of #3 was used as the anchorage point place a traction force on # 4 towards the buccal (Figs. 8-12). Tooth #13 received a buccal hook due to its strong rota-tion but there was enough available exposed crown to allow it to be tractioned from the anchored buccal hook on #14. The mandibu-lar arch was treated with straight arch wire sequence progressing 34 Summer 2023 JAOS
Journal of the American Orthodontic Society Summer 2023: Page 34