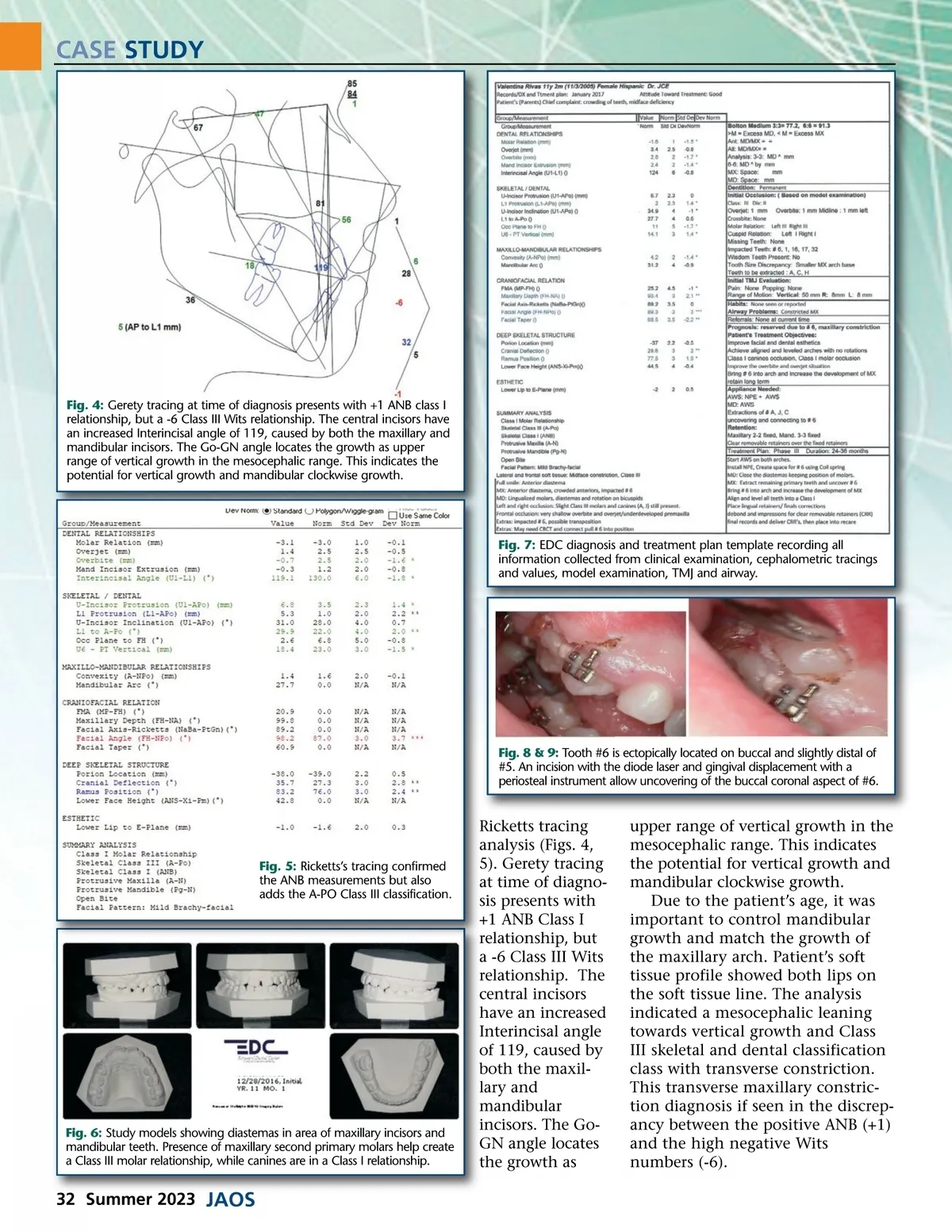
CASE STUDY Fig. 10a: Tooth #6 is ectopically located on buccal and slightly distal of #5. An incision with the diode laser and gingival displacement with a periosteal instrument allow uncovering of the buccal coronal aspect of #6. Fig. 10b: Tooth # 4 is cleaned and prepared for a bonded custom fabricated hook using .014 ligature wire and bonded flowable composite. Fig. 11: Teeth #6 and #4 have bonded buccal hooks and the extended arm of the Nitanium expander has been bent and modified with flowable composite to allow proper directional traction. Diagnosis • Class I skeletal ANB • Class III Wits, A-Po • Class III molar, Class I canine dental classification • Maxillary underdeveloped arch • Transposition in the eruption posi-tion of #5 and #6 with ectopic impacted position of #6 • Mandibular diastemas on anterior teeth • Rotation of #5, #21 • Maxillary diastema between incisors with poor alignment of these segment • Open bite tendency with vertical face growth factor Treatment Objectives • Eliminate poor dental alignment and achieve balanced dental occlusion in Class I relationship. • Transverse expansion of maxillary arch to stimulate maxillary growth for better relationship with the mandibular arch. • Improve the overjet and overbite and avoid anterior crossbite rela-tionship. • Eliminate the transposition of #5 and #6 bringing the canine into its proper position. • • • • • tional mini twin block brackets. Maxillary arch will be expanded using an adjustable NiTi expander. This expander will also be used as anchorage unit to help move and direct teeth #4 and #6 into the desired position. Extractions of primary teeth and surgical exposure with attach-ment of guidance devices to move the designated teeth (#4, #6) into the desired position. Straight wire technique in a .018 slot with conventional mini twin block brackets combined with the NPE expander on maxillary arch to finalize dental positioning and alignment. Class III interarch short pull elas-tics to stimulate growth of the maxilla in the anterior direction and redirect mandibular growth, achieving Class I molar occlusion and improved arch relationships. Fixed and removable retention. Estimated Treatment Time Active treatment will take approxi-mately 36 months, followed by super-vised orthodontic retention. The esti-mated time is extended due to canine impaction and transposition. Case Summary & Analysis At 11 years of age at time of orthodontic treatment, VR’s chief complaint was the impaction of her right permanent maxillary canine and the poor alignment of the maxil-lary incisors (Fig. 1). Comprehensive Treatment Plan • Mandibular arch will be treated with straight wire tech-nique in a .018 slot with conven-examination included hard and soft tissues, medical and dental issues (none), dental and skeletal classifica-tion (Class III) and an initial clinical impression of need of extraction of the primary teeth, expansion of the maxillary arch and management of the transposition of # 5 and #6. Patient was scheduled for orthodontic records including photographic images, panoramic and cephalometric images. These records were turned over to the author for comprehensive evalua-tion, diagnosis and treatment plan-ning. This process was documented in the EDC diagnosis and treatment template (Fig. 7), including all necessary observations obtained during clinical, radiographic and orthodontic evaluations, including treatment options and other proce-dures required to carry out the treatment, such as extractions, etc. Patient and parents were scheduled for presentation of findings, diagno-sis and treatment options. Presentation was done, questions answered including treatment options, and consent for treatment was obtained. That was followed by placement of separators to allow bands for maxillary arch and place-ment of a prefabricated NPE expander. Treatment started with cementa-tion of bands on all first molars, and www.orthodontics.com Summer 2023 33
Journal of the American Orthodontic Society Summer 2023: Page 33