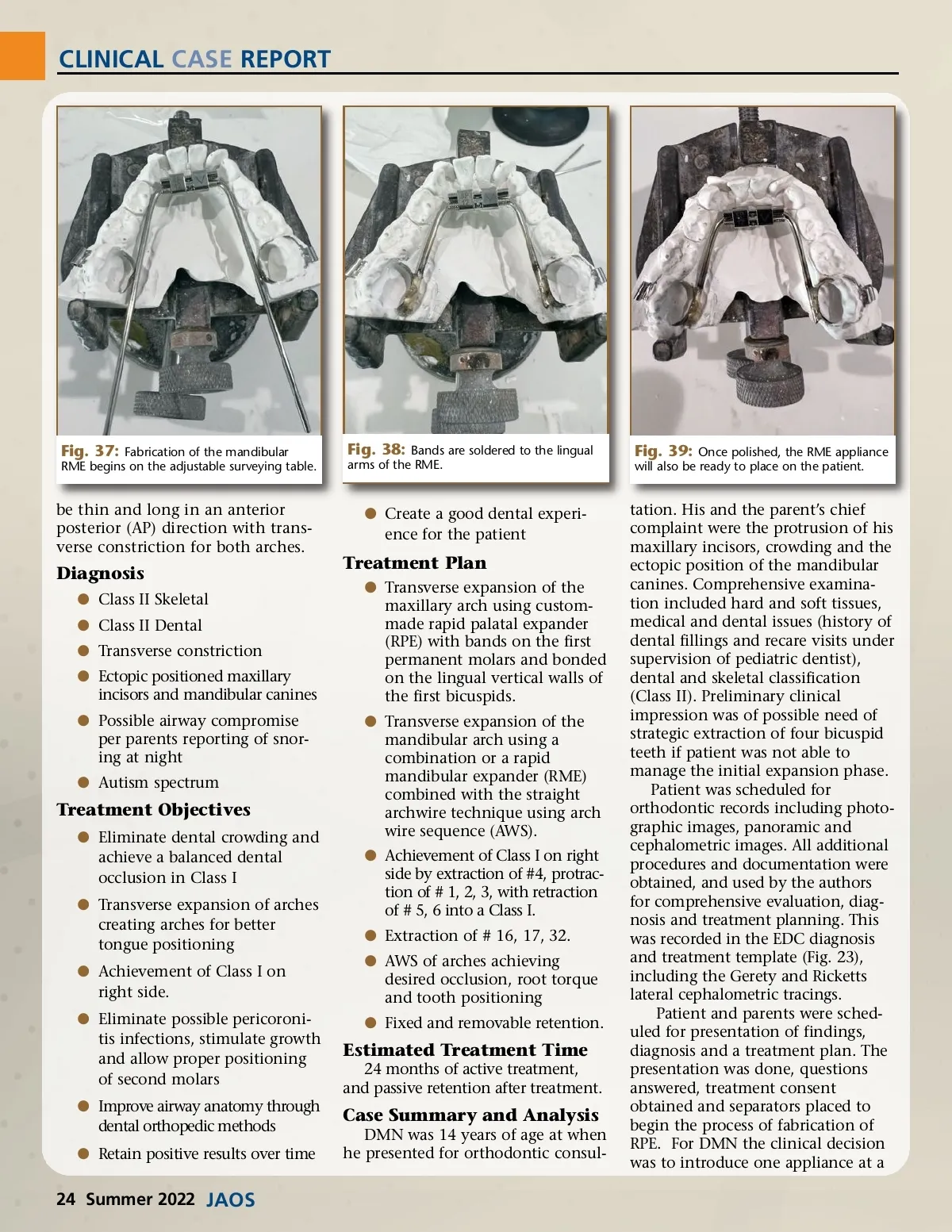
CLINICAL CASE REPORT Fig. 37: Fabrication of the mandibular RME begins on the adjustable surveying table. Fig. 38: Bands are soldered to the lingual arms of the RME. Fig. 39: Once polished, the RME appliance will also be ready to place on the patient. be thin and long in an anterior posterior (AP) direction with trans-verse constriction for both arches. b Create a good dental experi-ence for the patient Diagnosis b Class II Skeletal b Class II Dental b Transverse constriction b Ectopic positioned maxillary incisors and mandibular canines b Possible airway compromise per parents reporting of snor-ing at night b Autism spectrum Treatment Plan b Transverse expansion of the maxillary arch using custom-made rapid palatal expander (RPE) with bands on the first permanent molars and bonded on the lingual vertical walls of the first bicuspids. b Transverse expansion of the mandibular arch using a combination or a rapid mandibular expander (RME) combined with the straight archwire technique using arch wire sequence (AWS). b Achievement of Class I on right side by extraction of #4, protrac-tion of # 1, 2, 3, with retraction of # 5, 6 into a Class I. b Extraction of # 16, 17, 32. b AWS of arches achieving desired occlusion, root torque and tooth positioning b Fixed and removable retention. Treatment Objectives b Eliminate dental crowding and achieve a balanced dental occlusion in Class I b Transverse expansion of arches creating arches for better tongue positioning b Achievement of Class I on right side. b Eliminate possible pericoroni-tis infections, stimulate growth and allow proper positioning of second molars b Improve airway anatomy through dental orthopedic methods b Retain positive results over time Estimated Treatment Time 24 months of active treatment, and passive retention after treatment. Case Summary and Analysis DMN was 14 years of age at when he presented for orthodontic consul-tation. His and the parent’s chief complaint were the protrusion of his maxillary incisors, crowding and the ectopic position of the mandibular canines. Comprehensive examina-tion included hard and soft tissues, medical and dental issues (history of dental fillings and recare visits under supervision of pediatric dentist), dental and skeletal classification (Class II). Preliminary clinical impression was of possible need of strategic extraction of four bicuspid teeth if patient was not able to manage the initial expansion phase. Patient was scheduled for orthodontic records including photo-graphic images, panoramic and cephalometric images. All additional procedures and documentation were obtained, and used by the authors for comprehensive evaluation, diag-nosis and treatment planning. This was recorded in the EDC diagnosis and treatment template (Fig. 23), including the Gerety and Ricketts lateral cephalometric tracings. Patient and parents were sched-uled for presentation of findings, diagnosis and a treatment plan. The presentation was done, questions answered, treatment consent obtained and separators placed to begin the process of fabrication of RPE. For DMN the clinical decision was to introduce one appliance at a 24 Summer 2022 JAOS
Journal of the American Orthodontic Society Summer 2022: Page 24