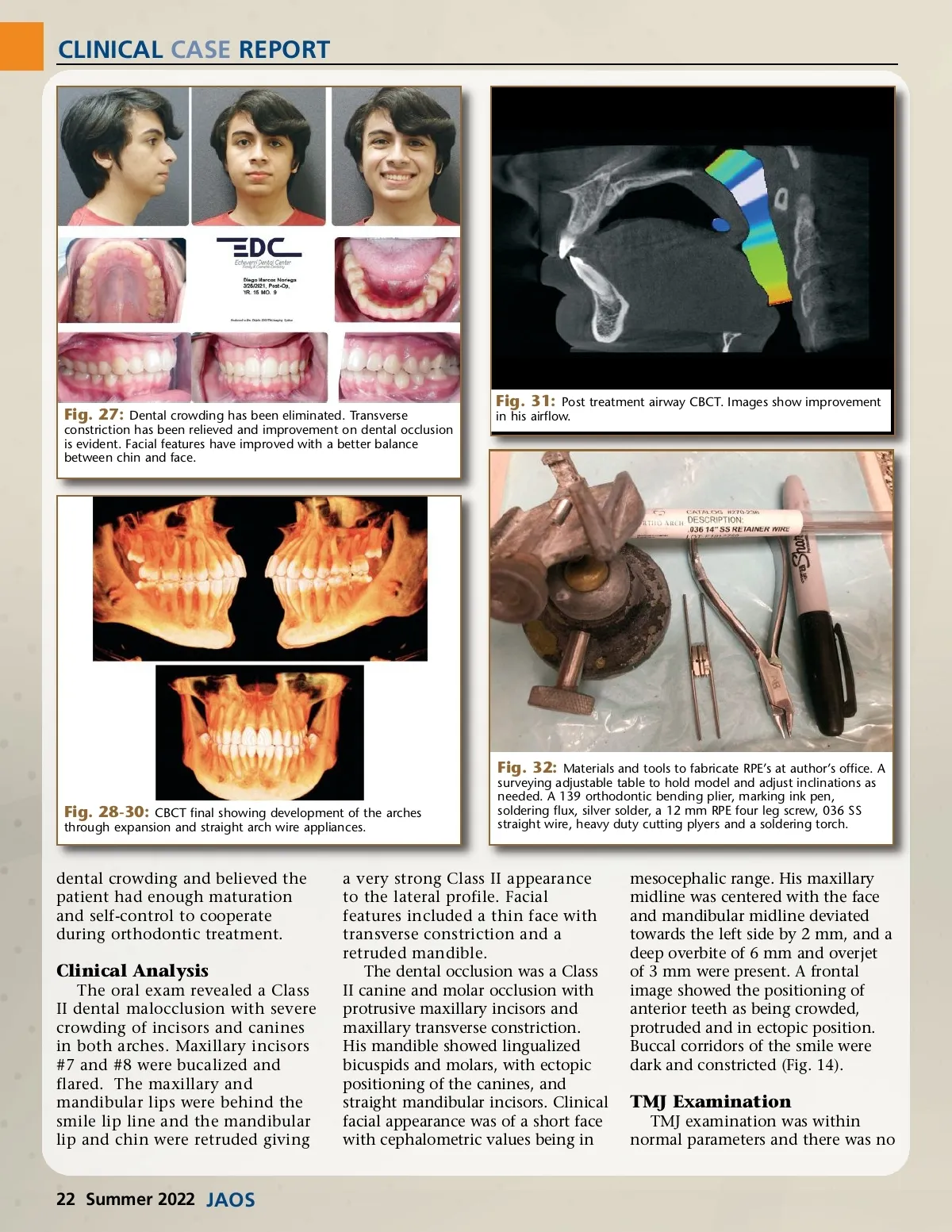
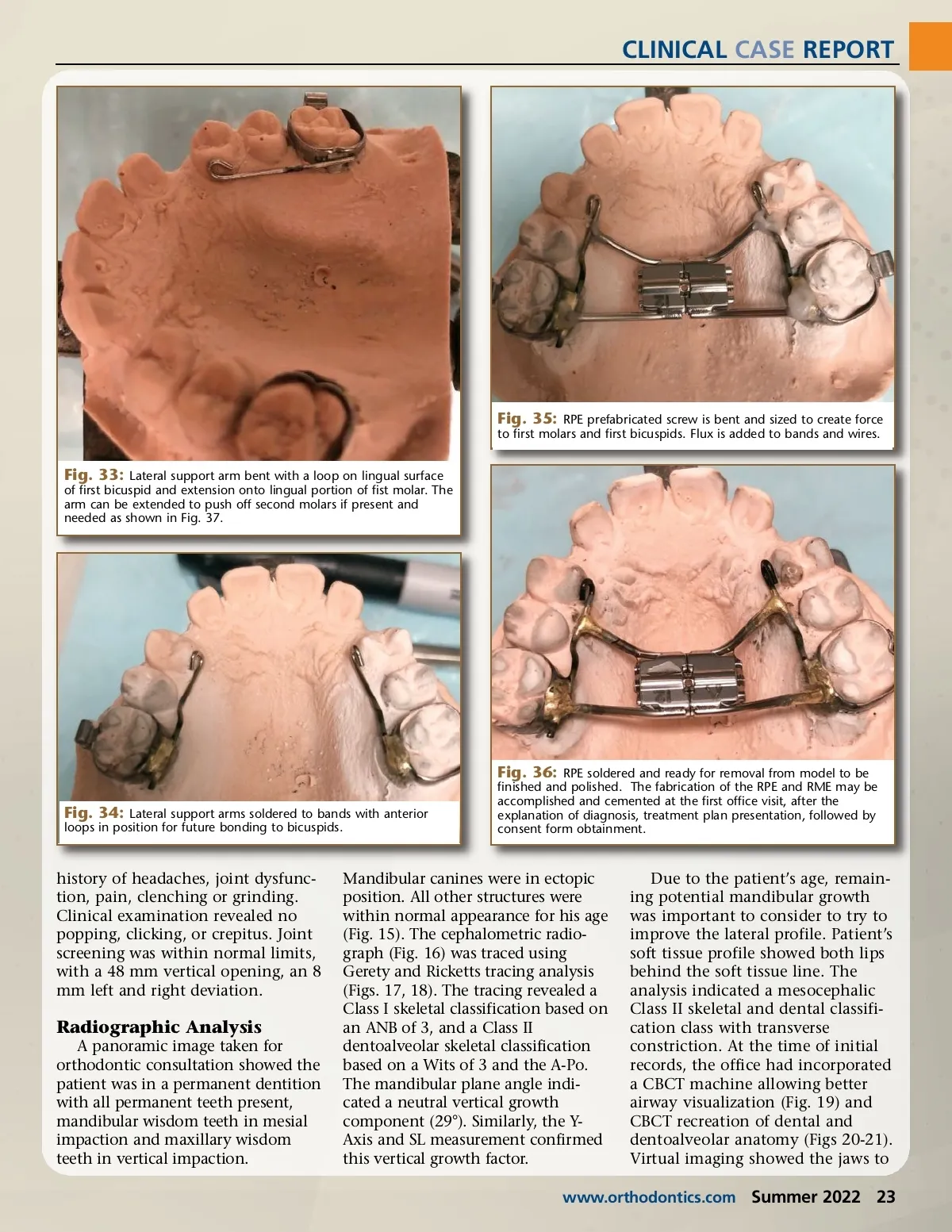
CLINICAL CASE REPORT Fig. 35: RPE prefabricated screw is bent and sized to create force to first molars and first bicuspids. Flux is added to bands and wires. Fig. 33: Lateral support arm bent with a loop on lingual surface of first bicuspid and extension onto lingual portion of fist molar. The arm can be extended to push off second molars if present and needed as shown in Fig. 37. Fig. 36: RPE soldered and ready for removal from model to be Fig. 34: Lateral support arms soldered to bands with anterior loops in position for future bonding to bicuspids. finished and polished. The fabrication of the RPE and RME may be accomplished and cemented at the first office visit, after the explanation of diagnosis, treatment plan presentation, followed by consent form obtainment. history of headaches, joint dysfunc-tion, pain, clenching or grinding. Clinical examination revealed no popping, clicking, or crepitus. Joint screening was within normal limits, with a 48 mm vertical opening, an 8 mm left and right deviation. Radiographic Analysis A panoramic image taken for orthodontic consultation showed the patient was in a permanent dentition with all permanent teeth present, mandibular wisdom teeth in mesial impaction and maxillary wisdom teeth in vertical impaction. Mandibular canines were in ectopic position. All other structures were within normal appearance for his age (Fig. 15). The cephalometric radio-graph (Fig. 16) was traced using Gerety and Ricketts tracing analysis (Figs. 17, 18). The tracing revealed a Class I skeletal classification based on an ANB of 3, and a Class II dentoalveolar skeletal classification based on a Wits of 3 and the A-Po. The mandibular plane angle indi-cated a neutral vertical growth component (29°). Similarly, the Y-Axis and SL measurement confirmed this vertical growth factor. Due to the patient’s age, remain-ing potential mandibular growth was important to consider to try to improve the lateral profile. Patient’s soft tissue profile showed both lips behind the soft tissue line. The analysis indicated a mesocephalic Class II skeletal and dental classifi-cation class with transverse constriction. At the time of initial records, the office had incorporated a CBCT machine allowing better airway visualization (Fig. 19) and CBCT recreation of dental and dentoalveolar anatomy (Figs 20-21). Virtual imaging showed the jaws to www.orthodontics.com Summer 2022 23
Journal of the American Orthodontic Society Summer 2022: Page 23