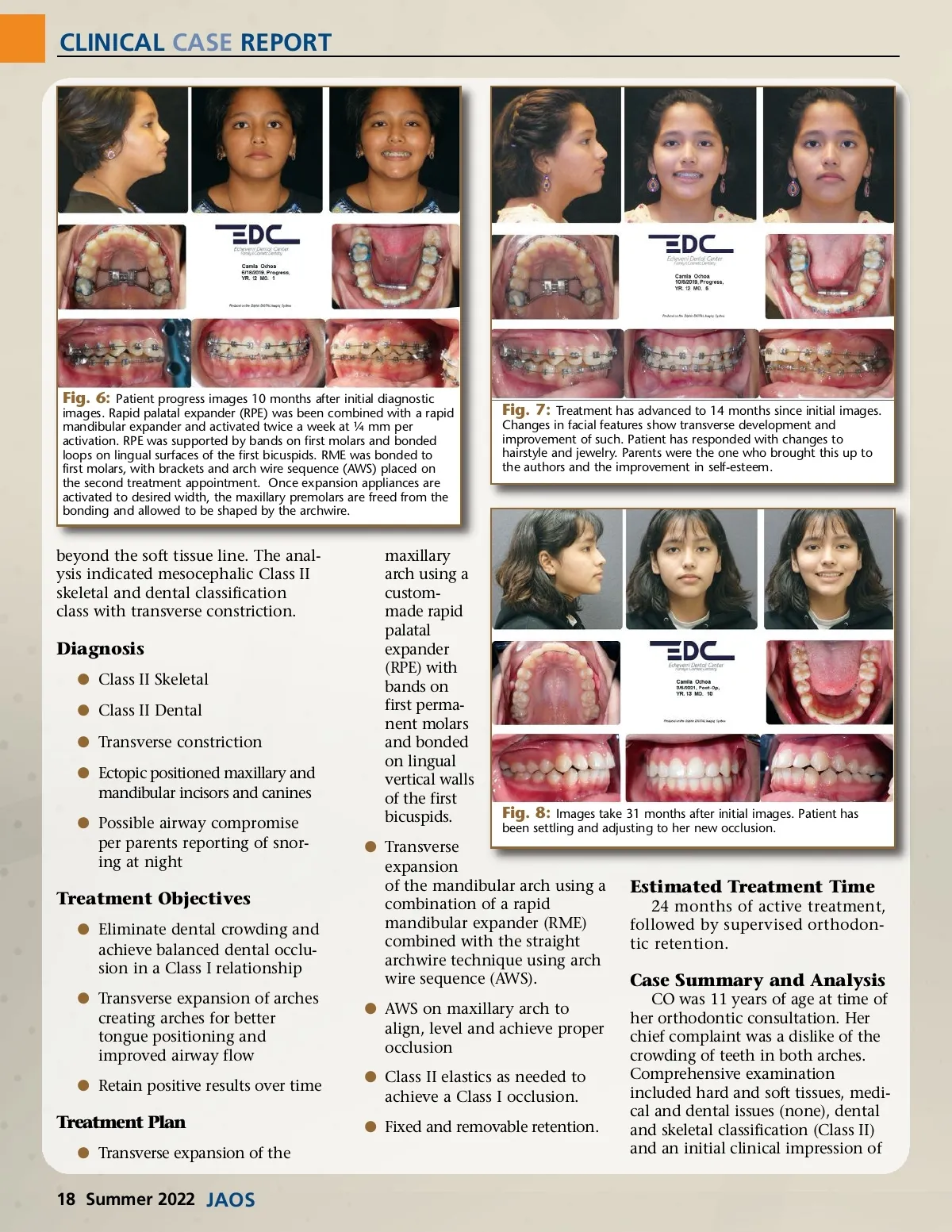
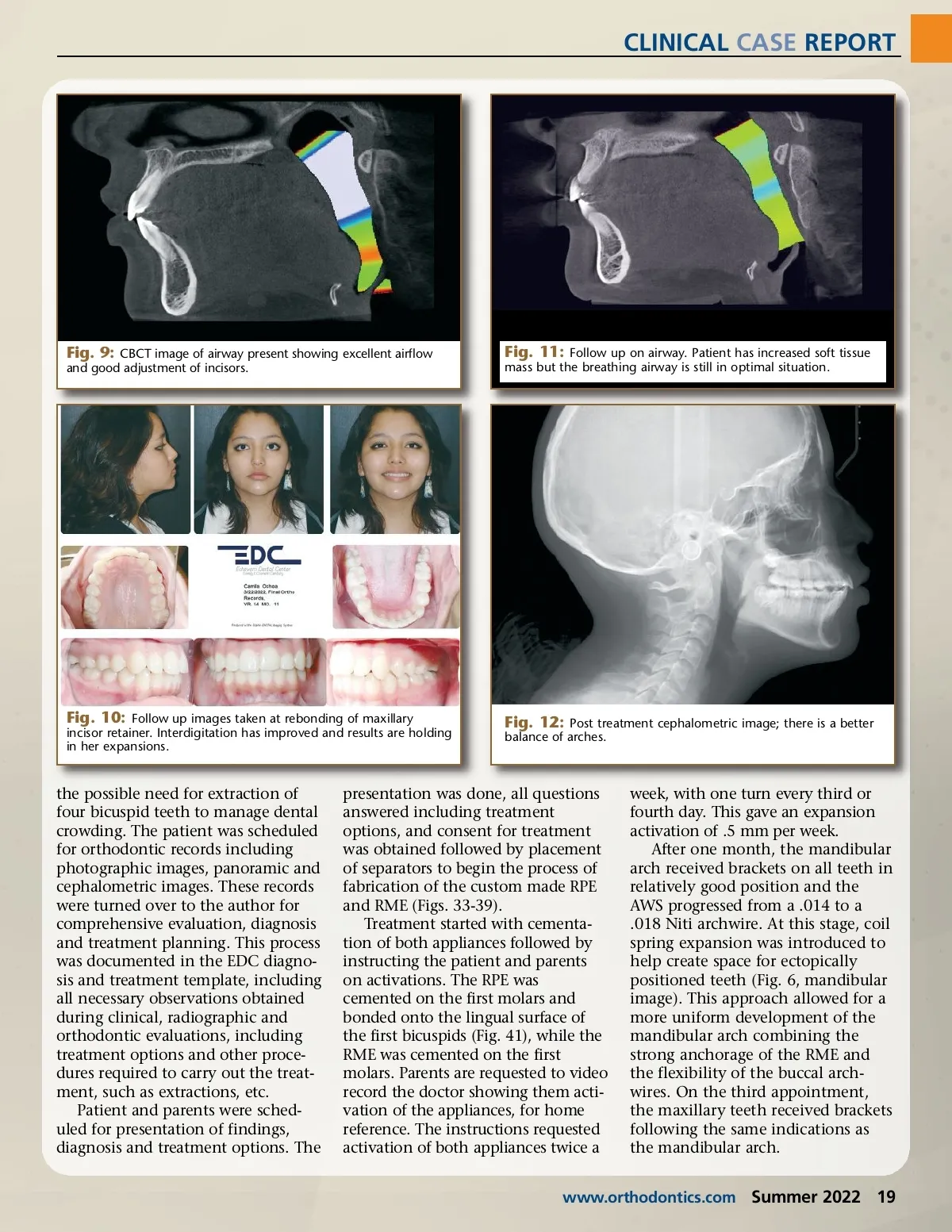
CLINICAL CASE REPORT Fig. 9: CBCT image of airway present showing excellent airflow and good adjustment of incisors. Fig. 11: Follow up on airway. Patient has increased soft tissue mass but the breathing airway is still in optimal situation. Fig. 10: Follow up images taken at rebonding of maxillary incisor retainer. Interdigitation has improved and results are holding in her expansions. Fig. 12: Post treatment cephalometric image; there is a better balance of arches. the possible need for extraction of four bicuspid teeth to manage dental crowding. The patient was scheduled for orthodontic records including photographic images, panoramic and cephalometric images. These records were turned over to the author for comprehensive evaluation, diagnosis and treatment planning. This process was documented in the EDC diagno-sis and treatment template, including all necessary observations obtained during clinical, radiographic and orthodontic evaluations, including treatment options and other proce-dures required to carry out the treat-ment, such as extractions, etc. Patient and parents were sched-uled for presentation of findings, diagnosis and treatment options. The presentation was done, all questions answered including treatment options, and consent for treatment was obtained followed by placement of separators to begin the process of fabrication of the custom made RPE and RME (Figs. 33-39). Treatment started with cementa-tion of both appliances followed by instructing the patient and parents on activations. The RPE was cemented on the first molars and bonded onto the lingual surface of the first bicuspids (Fig. 41), while the RME was cemented on the first molars. Parents are requested to video record the doctor showing them acti-vation of the appliances, for home reference. The instructions requested activation of both appliances twice a week, with one turn every third or fourth day. This gave an expansion activation of .5 mm per week. After one month, the mandibular arch received brackets on all teeth in relatively good position and the AWS progressed from a .014 to a .018 Niti archwire. At this stage, coil spring expansion was introduced to help create space for ectopically positioned teeth (Fig. 6, mandibular image). This approach allowed for a more uniform development of the mandibular arch combining the strong anchorage of the RME and the flexibility of the buccal arch-wires. On the third appointment, the maxillary teeth received brackets following the same indications as the mandibular arch. www.orthodontics.com Summer 2022 19
Journal of the American Orthodontic Society Summer 2022: Page 19