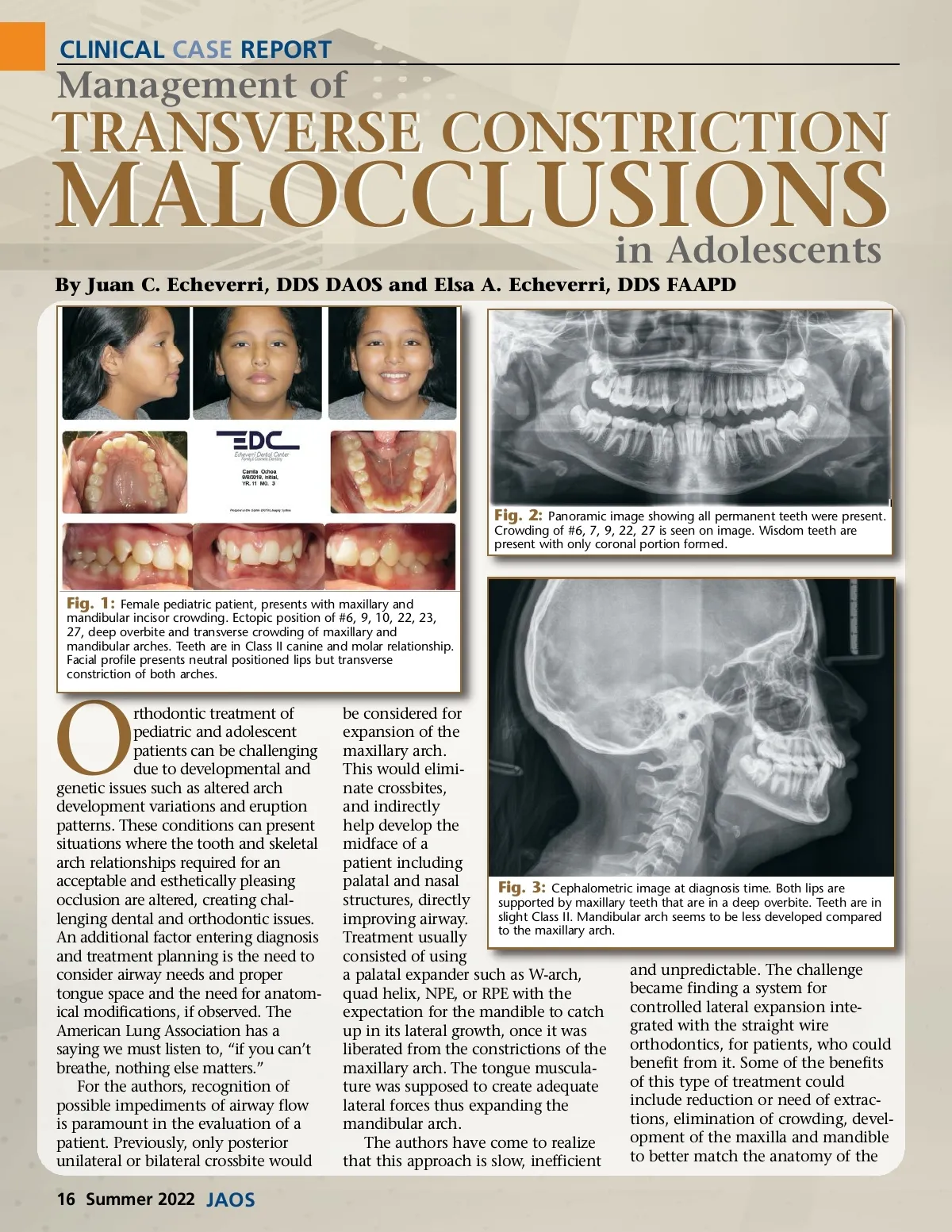
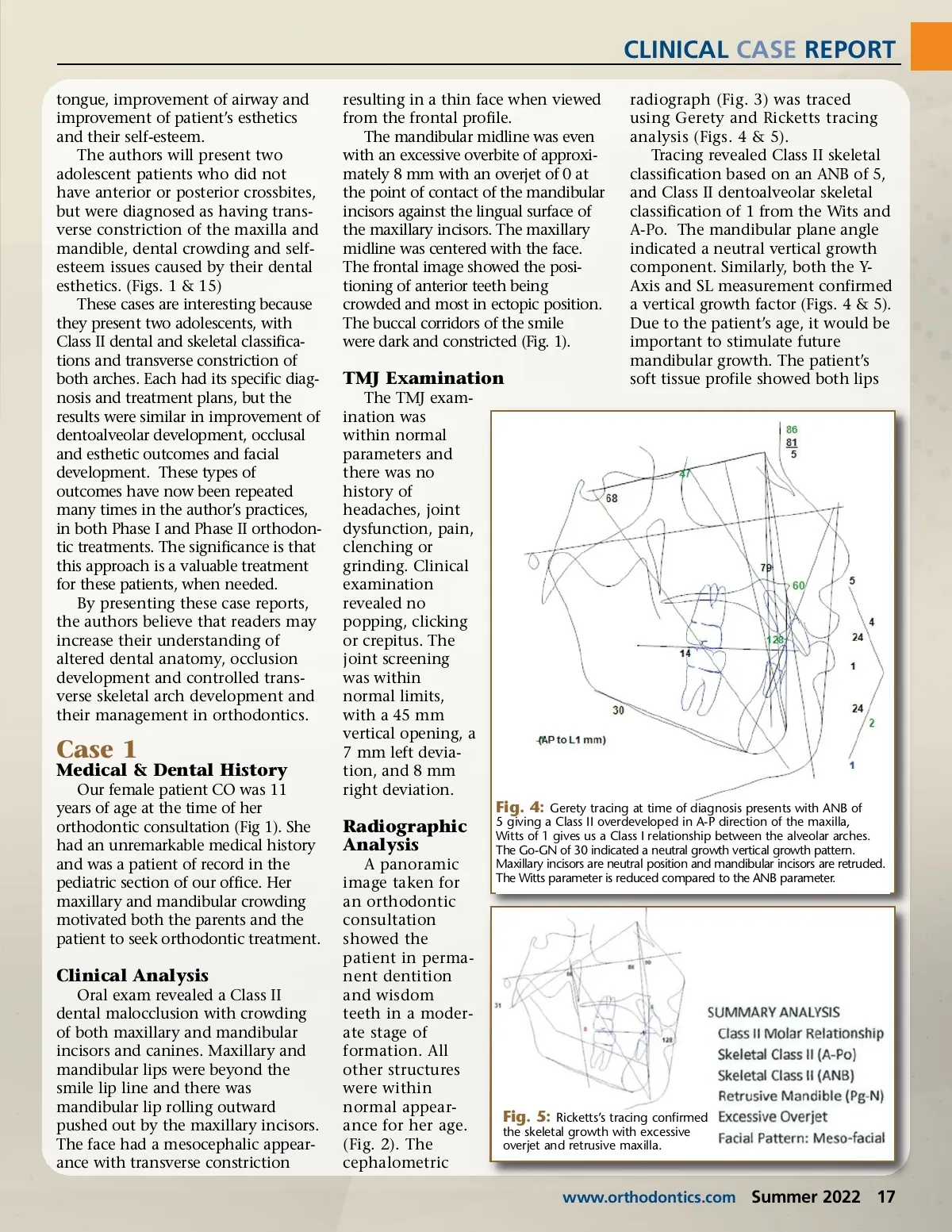
CLINICAL CASE REPORT tongue, improvement of airway and improvement of patient’s esthetics and their self-esteem. The authors will present two adolescent patients who did not have anterior or posterior crossbites, but were diagnosed as having trans-verse constriction of the maxilla and mandible, dental crowding and self-esteem issues caused by their dental esthetics. (Figs. 1 & 15) These cases are interesting because they present two adolescents, with Class II dental and skeletal classifica-tions and transverse constriction of both arches. Each had its specific diag-nosis and treatment plans, but the results were similar in improvement of dentoalveolar development, occlusal and esthetic outcomes and facial development. These types of outcomes have now been repeated many times in the author’s practices, in both Phase I and Phase II orthodon-tic treatments. The significance is that this approach is a valuable treatment for these patients, when needed. By presenting these case reports, the authors believe that readers may increase their understanding of altered dental anatomy, occlusion development and controlled trans-verse skeletal arch development and their management in orthodontics. resulting in a thin face when viewed from the frontal profile. The mandibular midline was even with an excessive overbite of approxi-mately 8 mm with an overjet of 0 at the point of contact of the mandibular incisors against the lingual surface of the maxillary incisors. The maxillary midline was centered with the face. The frontal image showed the posi-tioning of anterior teeth being crowded and most in ectopic position. The buccal corridors of the smile were dark and constricted (Fig. 1). radiograph (Fig. 3) was traced using Gerety and Ricketts tracing analysis (Figs. 4 & 5). Tracing revealed Class II skeletal classification based on an ANB of 5, and Class II dentoalveolar skeletal classification of 1 from the Wits and A-Po. The mandibular plane angle indicated a neutral vertical growth component. Similarly, both the Y-Axis and SL measurement confirmed a vertical growth factor (Figs. 4 & 5). Due to the patient’s age, it would be important to stimulate future mandibular growth. The patient’s soft tissue profile showed both lips TMJ Examination The TMJ exam-ination was within normal parameters and there was no history of headaches, joint dysfunction, pain, clenching or grinding. Clinical examination revealed no popping, clicking or crepitus. The joint screening was within normal limits, with a 45 mm vertical opening, a 7 mm left devia-tion, and 8 mm right deviation. Case 1 Medical & Dental History Our female patient CO was 11 years of age at the time of her orthodontic consultation (Fig 1). She had an unremarkable medical history and was a patient of record in the pediatric section of our office. Her maxillary and mandibular crowding motivated both the parents and the patient to seek orthodontic treatment. Fig. 4: Gerety tracing at time of diagnosis presents with ANB of Radiographic Analysis A panoramic image taken for an orthodontic consultation showed the patient in perma-nent dentition and wisdom teeth in a moder-ate stage of formation. All other structures were within normal appear-ance for her age. (Fig. 2). The cephalometric 5 giving a Class II overdeveloped in A-P direction of the maxilla, Witts of 1 gives us a Class I relationship between the alveolar arches. The Go-GN of 30 indicated a neutral growth vertical growth pattern. Maxillary incisors are neutral position and mandibular incisors are retruded. The Witts parameter is reduced compared to the ANB parameter. Clinical Analysis Oral exam revealed a Class II dental malocclusion with crowding of both maxillary and mandibular incisors and canines. Maxillary and mandibular lips were beyond the smile lip line and there was mandibular lip rolling outward pushed out by the maxillary incisors. The face had a mesocephalic appear-ance with transverse constriction Fig. 5: Ricketts’s tracing confirmed the skeletal growth with excessive overjet and retrusive maxilla. www.orthodontics.com Summer 2022 17
Journal of the American Orthodontic Society Summer 2022: Page 17