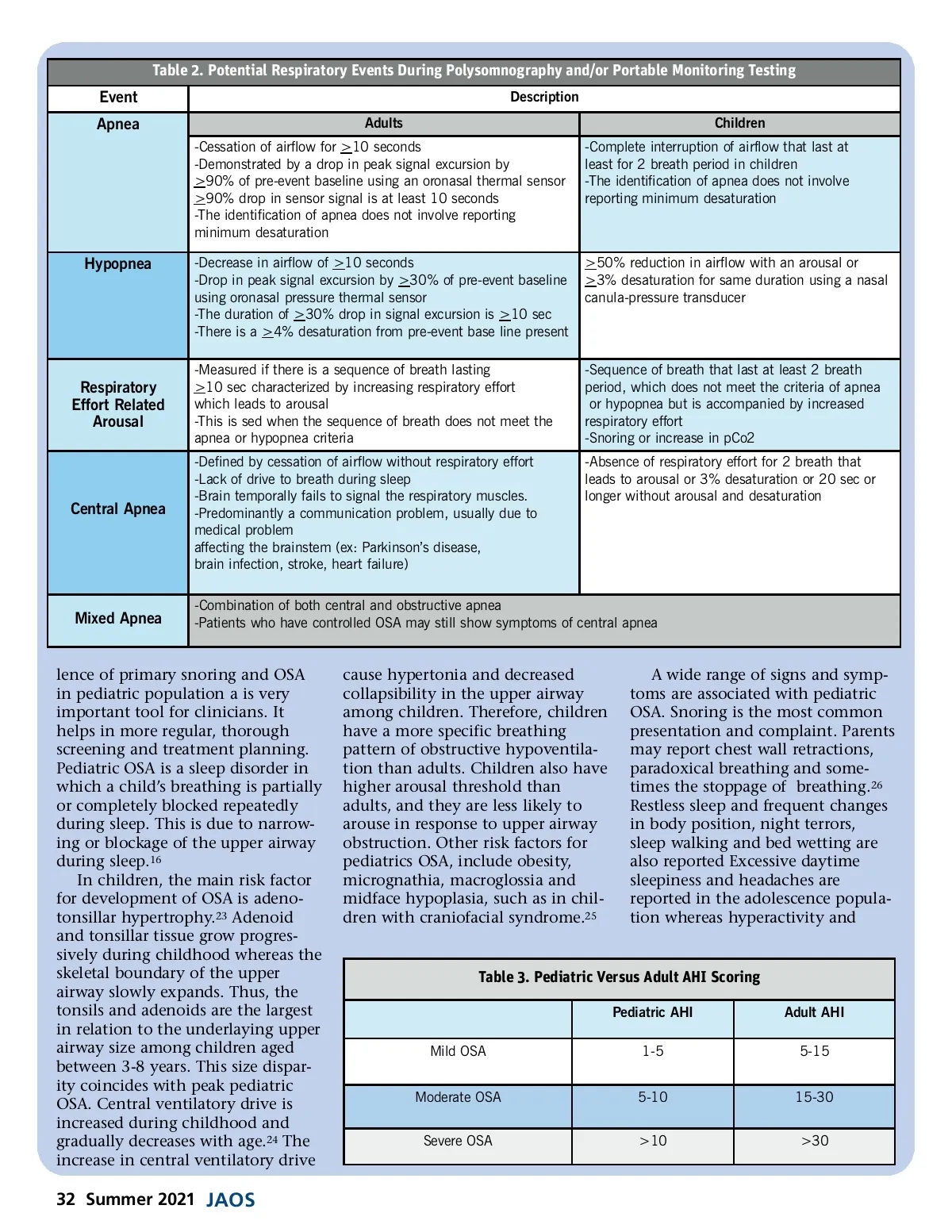
attention deficit reported in preado-lescent children with OSA. Untreated pediatric OSA can result in serious morbidity in neurobehav-ioral, cardiovascular, and somatic growth and development. 23 Many studies showed a clear association between OSA and hyperactivity, attention deficit, and other behav-ioral problems in children. The diagnosis of OSA in children is made on the basis of sleep history, physical examination, and polysomnography. A comprehen-sive physical exam of the upper airway from nose to pharynx can help to identify any obstruction or deviation of a nasal septum defect, hard and soft palate examination for narrowing, and assessment of tonsillar enlargement. Observation of tongue size and the use of the Mallampati scores 27 are helpful in evaluating the patency of the airway related to the tonsillar size. An adenoid face with mouth breathing during awake time is an important clue in detecting sleep-disorder breathing. Polysomnography is considered the only gold standard for diagnosis of pediatric OSA. 28 This test is performed in the lab and supervised by trained technician with addi-tional record keeping of unusual events or behavior during the night. In children end-tidal CO2 measure-ment is very important in diagnosis of OSA. This is particularly impor-tant in children with obesity and neuromuscular disease, who have a higher risk of hypoventilation. The PSG parameters that are most commonly used in pediatric OSA are AHI, REARA’s and RDI (Table 2). The first line of therapy for most children with OSA is adenotonsillec-tomy. 29 A rapid palatal expander can also be used in combination with surgery to further expand the palate if constriction exists. Potential complications may include postoper-ative bleeding, pain. In addition, some patients may develop respira-tory complications, therefore, overnight monitoring is required. In patients with surgical contraindications, minimal adeno-tonsillar hypertrophy, or persistence OSA, CPAP therapy is an option. In these children CPAP needs to be used indefinitely. Diagnosis of OSA in Adults The diagnosis of OSA is based upon the presence or absence of related symptoms as well as the frequency of respiratory events during sleep. Obtaining a detailed medical and sleep history is very important for determining the need and subtype of intervention. We can use many screening questioners such as the STOP-Bang question-naire that assesses snoring, the level of tiredness and fatigue, witnessed absence of breathing, total body mass index and neck circumference measurement. 30 The composite score in this screening tool will tell us about risk for OSA. Additionally, the Epworth sleepiness scale can also be used, which measures daytime sleepiness and is a risk factor for OSA as well. 31 The patient clinical examination is also a very important part for the diagnosis of OSA. Assessment of obstruction and/or allergy should be conducted beginning at the nasal passage. Likewise, the oral cavity should be assessed, and tongue size should be measured and classified using the Mallampati score. 27 While evaluating the oral cavity, dental signs of bruxism and anatomical hard and/or soft palate abnormalities should be noted. OSA is diagnosed by looking at the Apnea Hypopnea Index (AHI). 32 This ratio is a combination of obstructive apnea plus hypopnea plus central apnea plus mixed apnea. The AHI is used in combina-tion with daytime sleepiness to diagnose the severity of OSA and the lowest oxygen desaturation is reported as a part of the diagnosis. Additionally, the respiratory distur-bance index (RDI) can also be used to facilitate the diagnosis of OSA, and the RDI is a combination of the AHI and respiratory effort-related arousals (RERA). 33,34 The AHI ratio is used in combination with daytime sleepiness to diagnose the severity of OSA.(Table 3) Polysomnography (PSG) or Portable Monitoring In order to evaluate a patient’s breathing pattern during sleep, laboratory polysomnography (PSG) testing 35 or at-home testing through portable monitoring test should be conducted. The sleep study report looks at several different respiratory events (Table 2). Overall, these events include apnea, hypopnea, and respiratory effort-related arousals (RERA), central apnea and mixed apnea. Treatment of Adult OSA For decades the gold standard of care, beyond weight loss, was using CPAP 36 . This is a form of positive airway pressure ventilation in which a constant level of air pressure greater than atmospheric pressure is continuously applied to the upper respiratory track, which can prevent the collapse of the upper airway. 37 www.orthodontics.com Summer 2021 33
Journal of the American Orthodontic Society Summer 2021: Page 33