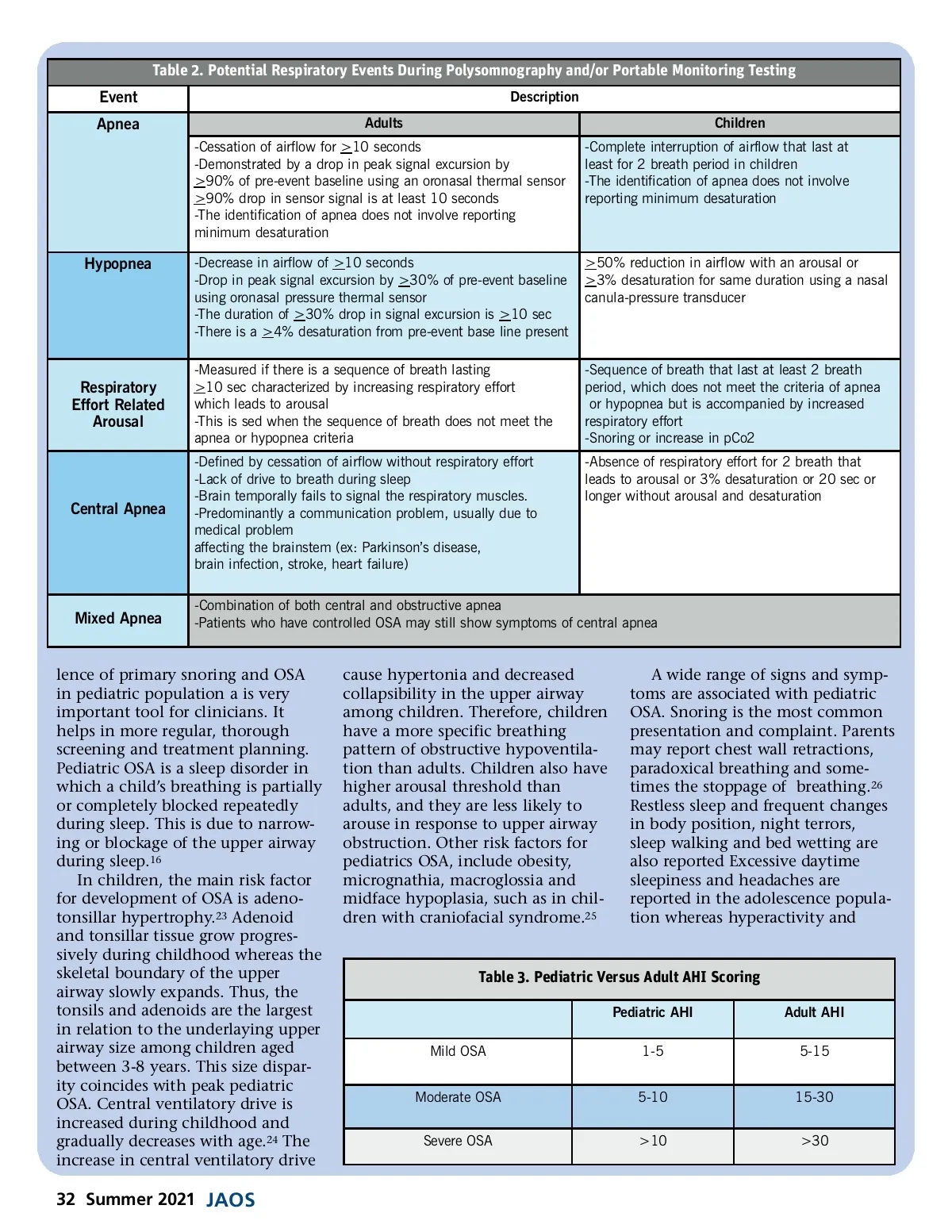
Table 2. Potential Respiratory Events During Polysomnography and/or Portable Monitoring Testing Event Apnea Adults -Cessation of airflow for >10 seconds -Demonstrated by a drop in peak signal excursion by >90% of pre-event baseline using an oronasal thermal sensor >90% drop in sensor signal is at least 10 seconds -The identification of apnea does not involve reporting minimum desaturation Description Children -Complete interruption of airflow that last at least for 2 breath period in children -The identification of apnea does not involve reporting minimum desaturation Hypopnea -Decrease in airflow of >10 seconds -Drop in peak signal excursion by >30% of pre-event baseline using oronasal pressure thermal sensor -The duration of >30% drop in signal excursion is >10 sec -There is a >4% desaturation from pre-event base line present -Measured if there is a sequence of breath lasting >10 sec characterized by increasing respiratory effort which leads to arousal -This is sed when the sequence of breath does not meet the apnea or hypopnea criteria -Defined by cessation of airflow without respiratory effort -Lack of drive to breath during sleep -Brain temporally fails to signal the respiratory muscles. -Predominantly a communication problem, usually due to medical problem affecting the brainstem (ex: Parkinson’s disease, brain infection, stroke, heart failure) >50% reduction in airflow with an arousal or >3% desaturation for same duration using a nasal canula-pressure transducer Respiratory Effort Related Arousal -Sequence of breath that last at least 2 breath period, which does not meet the criteria of apnea or hypopnea but is accompanied by increased respiratory effort -Snoring or increase in pCo2 -Absence of respiratory effort for 2 breath that leads to arousal or 3% desaturation or 20 sec or longer without arousal and desaturation Central Apnea Mixed Apnea -Combination of both central and obstructive apnea -Patients who have controlled OSA may still show symptoms of central apnea lence of primary snoring and OSA in pediatric population a is very important tool for clinicians. It helps in more regular, thorough screening and treatment planning. Pediatric OSA is a sleep disorder in which a child’s breathing is partially or completely blocked repeatedly during sleep. This is due to narrow-ing or blockage of the upper airway during sleep. 16 In children, the main risk factor for development of OSA is adeno-tonsillar hypertrophy. 23 Adenoid and tonsillar tissue grow progres-sively during childhood whereas the skeletal boundary of the upper airway slowly expands. Thus, the tonsils and adenoids are the largest in relation to the underlaying upper airway size among children aged between 3-8 years. This size dispar-ity coincides with peak pediatric OSA. Central ventilatory drive is increased during childhood and gradually decreases with age. 24 The increase in central ventilatory drive cause hypertonia and decreased collapsibility in the upper airway among children. Therefore, children have a more specific breathing pattern of obstructive hypoventila-tion than adults. Children also have higher arousal threshold than adults, and they are less likely to arouse in response to upper airway obstruction. Other risk factors for pediatrics OSA, include obesity, micrognathia, macroglossia and midface hypoplasia, such as in chil-dren with craniofacial syndrome. 25 A wide range of signs and symp-toms are associated with pediatric OSA. Snoring is the most common presentation and complaint. Parents may report chest wall retractions, paradoxical breathing and some-times the stoppage of breathing. 26 Restless sleep and frequent changes in body position, night terrors, sleep walking and bed wetting are also reported Excessive daytime sleepiness and headaches are reported in the adolescence popula-tion whereas hyperactivity and Table 3. Pediatric Versus Adult AHI Scoring Pediatric AHI Mild OSA Moderate OSA Severe OSA 1-5 5-10 >10 Adult AHI 5-15 15-30 >30 32 Summer 2021 JAOS
Journal of the American Orthodontic Society Summer 2021: Page 32