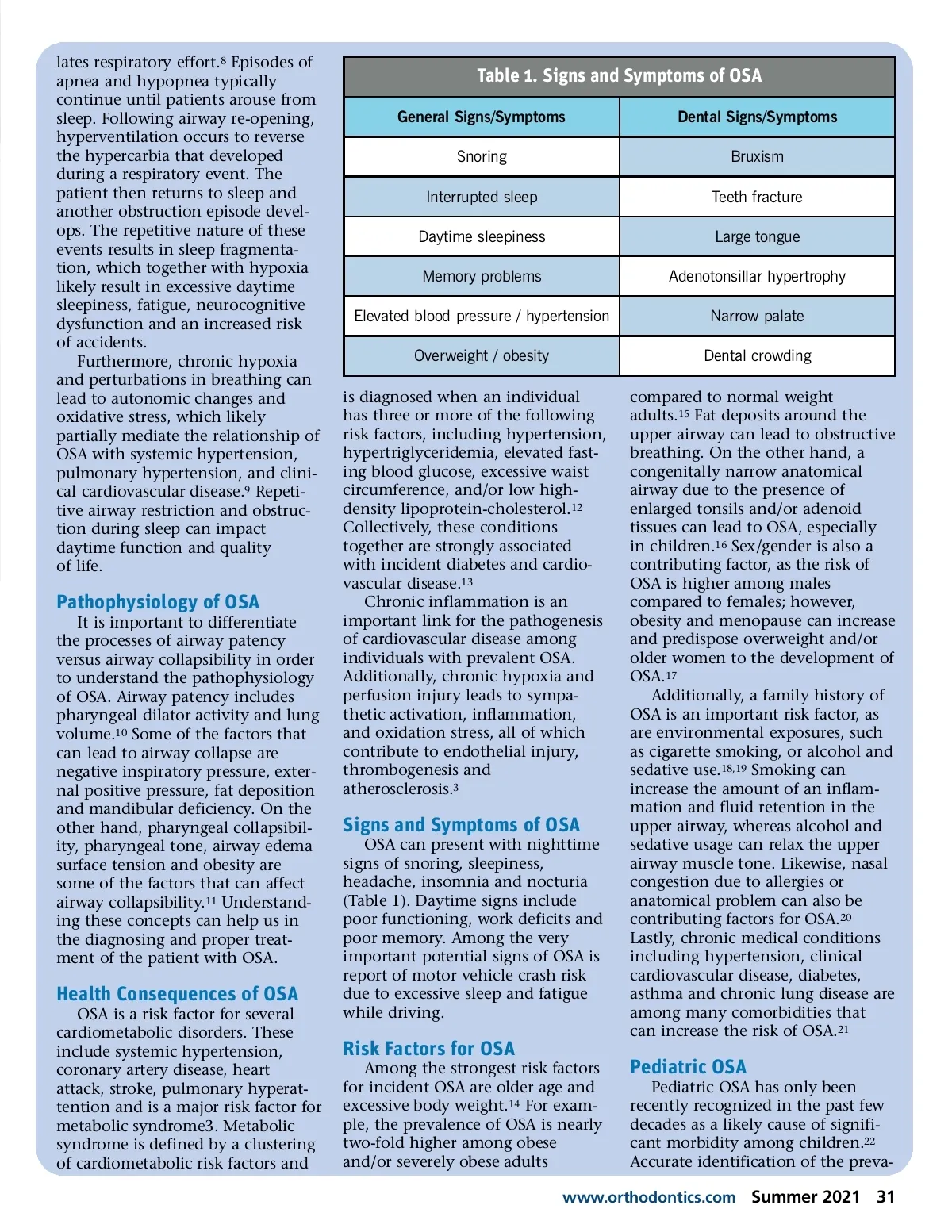
lates respiratory effort. 8 Episodes of apnea and hypopnea typically continue until patients arouse from sleep. Following airway re-opening, hyperventilation occurs to reverse the hypercarbia that developed during a respiratory event. The patient then returns to sleep and another obstruction episode devel-ops. The repetitive nature of these events results in sleep fragmenta-tion, which together with hypoxia likely result in excessive daytime sleepiness, fatigue, neurocognitive dysfunction and an increased risk of accidents. Furthermore, chronic hypoxia and perturbations in breathing can lead to autonomic changes and oxidative stress, which likely partially mediate the relationship of OSA with systemic hypertension, pulmonary hypertension, and clini-cal cardiovascular disease. 9 Repeti-tive airway restriction and obstruc-tion during sleep can impact daytime function and quality of life. Table 1. Signs and Symptoms of OSA General Signs/Symptoms Snoring Interrupted sleep Daytime sleepiness Memory problems Elevated blood pressure / hypertension Overweight / obesity is diagnosed when an individual has three or more of the following risk factors, including hypertension, hypertriglyceridemia, elevated fast-ing blood glucose, excessive waist circumference, and/or low high-density lipoprotein-cholesterol. 12 Collectively, these conditions together are strongly associated with incident diabetes and cardio-vascular disease. 13 Chronic inflammation is an important link for the pathogenesis of cardiovascular disease among individuals with prevalent OSA. Additionally, chronic hypoxia and perfusion injury leads to sympa-thetic activation, inflammation, and oxidation stress, all of which contribute to endothelial injury, thrombogenesis and atherosclerosis. 3 Dental Signs/Symptoms Bruxism Teeth fracture Large tongue Adenotonsillar hypertrophy Narrow palate Dental crowding compared to normal weight adults. 15 Fat deposits around the upper airway can lead to obstructive breathing. On the other hand, a congenitally narrow anatomical airway due to the presence of enlarged tonsils and/or adenoid tissues can lead to OSA, especially in children. 16 Sex/gender is also a contributing factor, as the risk of OSA is higher among males compared to females; however, obesity and menopause can increase and predispose overweight and/or older women to the development of OSA. 17 Additionally, a family history of OSA is an important risk factor, as are environmental exposures, such as cigarette smoking, or alcohol and sedative use. 18,19 Smoking can increase the amount of an inflam-mation and fluid retention in the upper airway, whereas alcohol and sedative usage can relax the upper airway muscle tone. Likewise, nasal congestion due to allergies or anatomical problem can also be contributing factors for OSA. 20 Lastly, chronic medical conditions including hypertension, clinical cardiovascular disease, diabetes, asthma and chronic lung disease are among many comorbidities that can increase the risk of OSA. 21 Pathophysiology of OSA It is important to differentiate the processes of airway patency versus airway collapsibility in order to understand the pathophysiology of OSA. Airway patency includes pharyngeal dilator activity and lung volume. 10 Some of the factors that can lead to airway collapse are negative inspiratory pressure, exter-nal positive pressure, fat deposition and mandibular deficiency. On the other hand, pharyngeal collapsibil-ity, pharyngeal tone, airway edema surface tension and obesity are some of the factors that can affect airway collapsibility. 11 Understand-ing these concepts can help us in the diagnosing and proper treat-ment of the patient with OSA. Signs and Symptoms of OSA OSA can present with nighttime signs of snoring, sleepiness, headache, insomnia and nocturia (Table 1). Daytime signs include poor functioning, work deficits and poor memory. Among the very important potential signs of OSA is report of motor vehicle crash risk due to excessive sleep and fatigue while driving. Health Consequences of OSA OSA is a risk factor for several cardiometabolic disorders. These include systemic hypertension, coronary artery disease, heart attack, stroke, pulmonary hyperat-tention and is a major risk factor for metabolic syndrome3. Metabolic syndrome is defined by a clustering of cardiometabolic risk factors and Risk Factors for OSA Among the strongest risk factors for incident OSA are older age and excessive body weight. 14 For exam-ple, the prevalence of OSA is nearly two-fold higher among obese and/or severely obese adults Pediatric OSA Pediatric OSA has only been recently recognized in the past few decades as a likely cause of signifi-cant morbidity among children. 22 Accurate identification of the preva-www.orthodontics.com Summer 2021 31
Journal of the American Orthodontic Society Summer 2021: Page 31