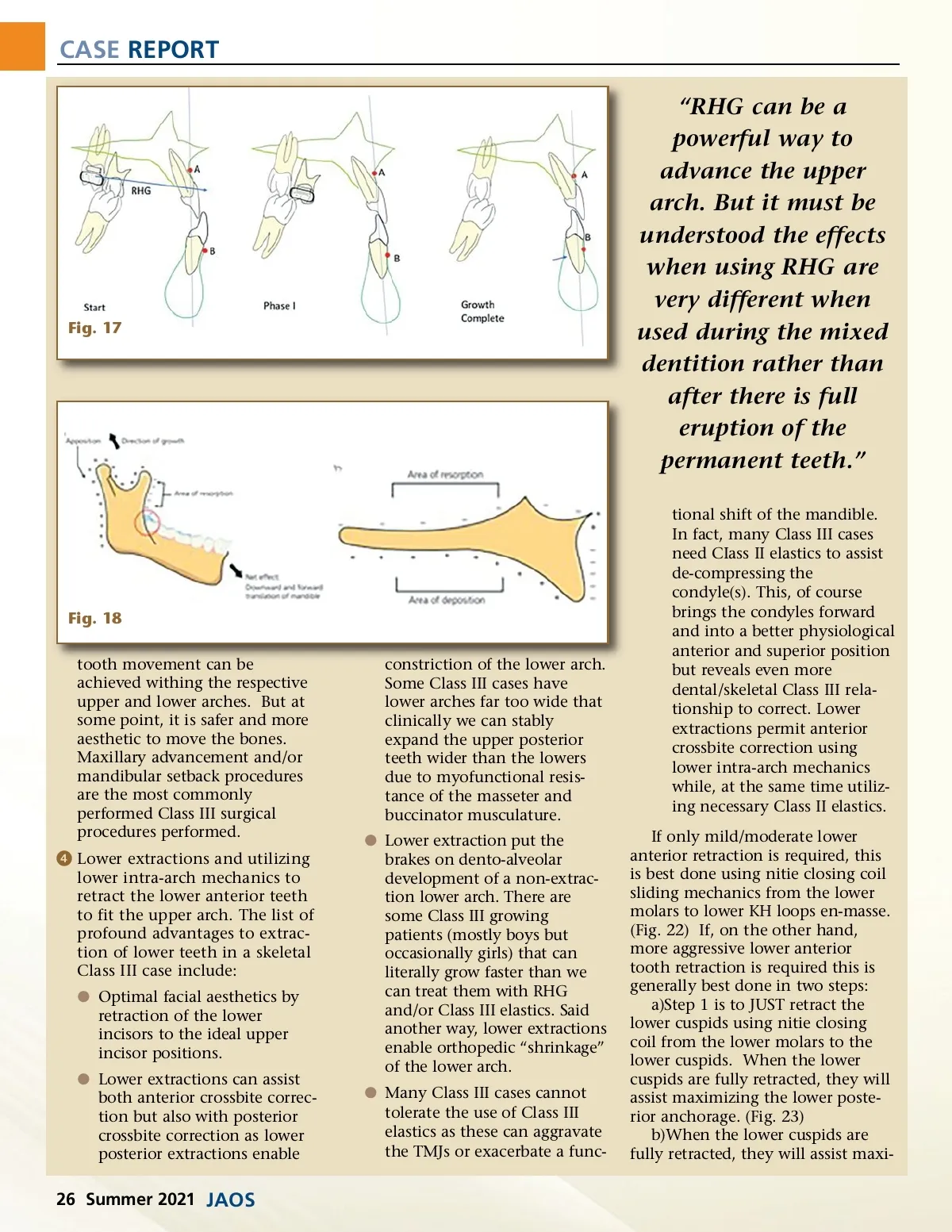
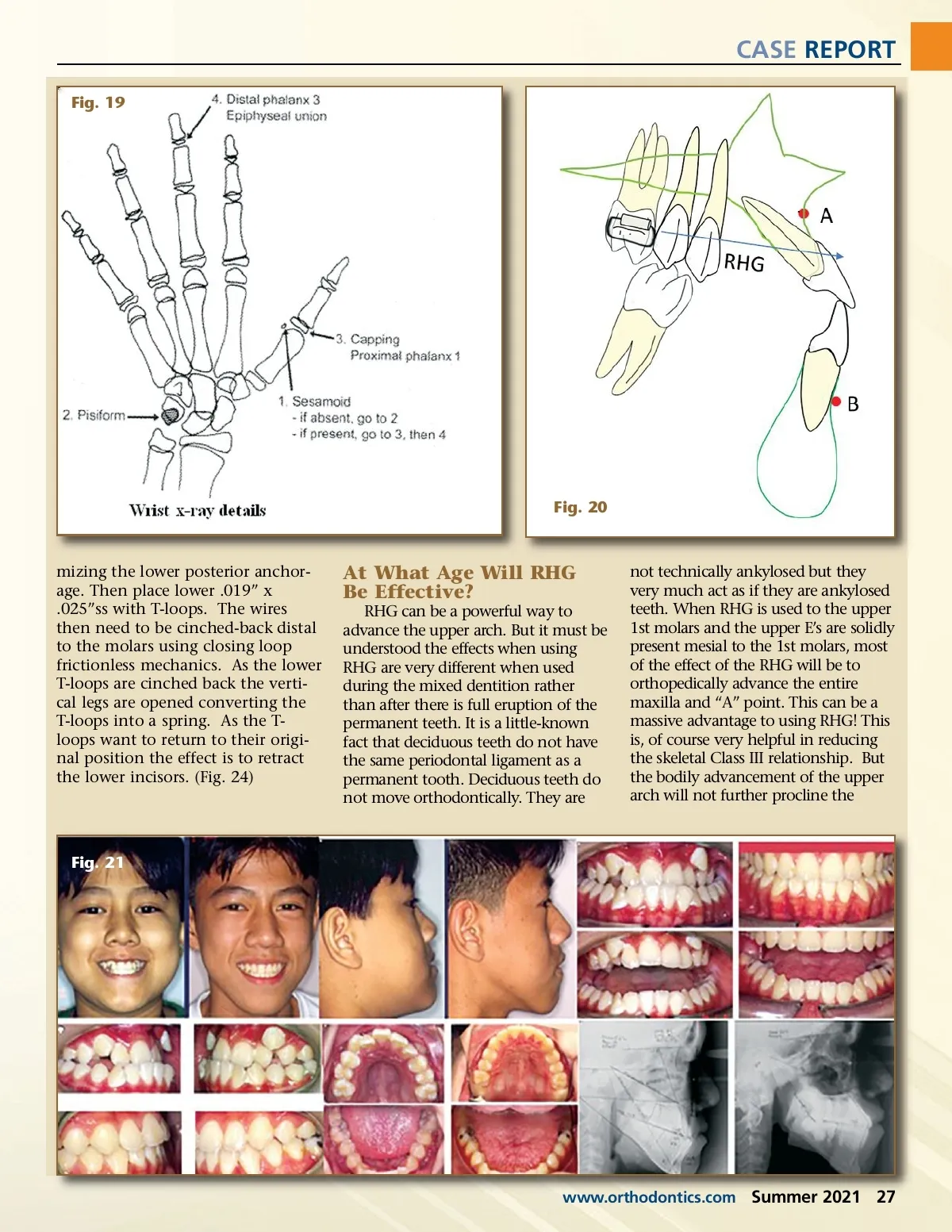
CASE REPORT Fig. 19 Fig. 20 mizing the lower posterior anchor-age. Then place lower .019” x .025”ss with T-loops. The wires then need to be cinched-back distal to the molars using closing loop frictionless mechanics. As the lower T-loops are cinched back the verti-cal legs are opened converting the T-loops into a spring. As the T-loops want to return to their origi-nal position the effect is to retract the lower incisors. (Fig. 24) At What Age Will RHG Be Effective? RHG can be a powerful way to advance the upper arch. But it must be understood the effects when using RHG are very different when used during the mixed dentition rather than after there is full eruption of the permanent teeth. It is a little-known fact that deciduous teeth do not have the same periodontal ligament as a permanent tooth. Deciduous teeth do not move orthodontically. They are not technically ankylosed but they very much act as if they are ankylosed teeth. When RHG is used to the upper 1st molars and the upper E’s are solidly present mesial to the 1st molars, most of the effect of the RHG will be to orthopedically advance the entire maxilla and “A” point. This can be a massive advantage to using RHG! This is, of course very helpful in reducing the skeletal Class III relationship. But the bodily advancement of the upper arch will not further procline the Fig. 21 www.orthodontics.com Summer 2021 27
Journal of the American Orthodontic Society Summer 2021: Page 27