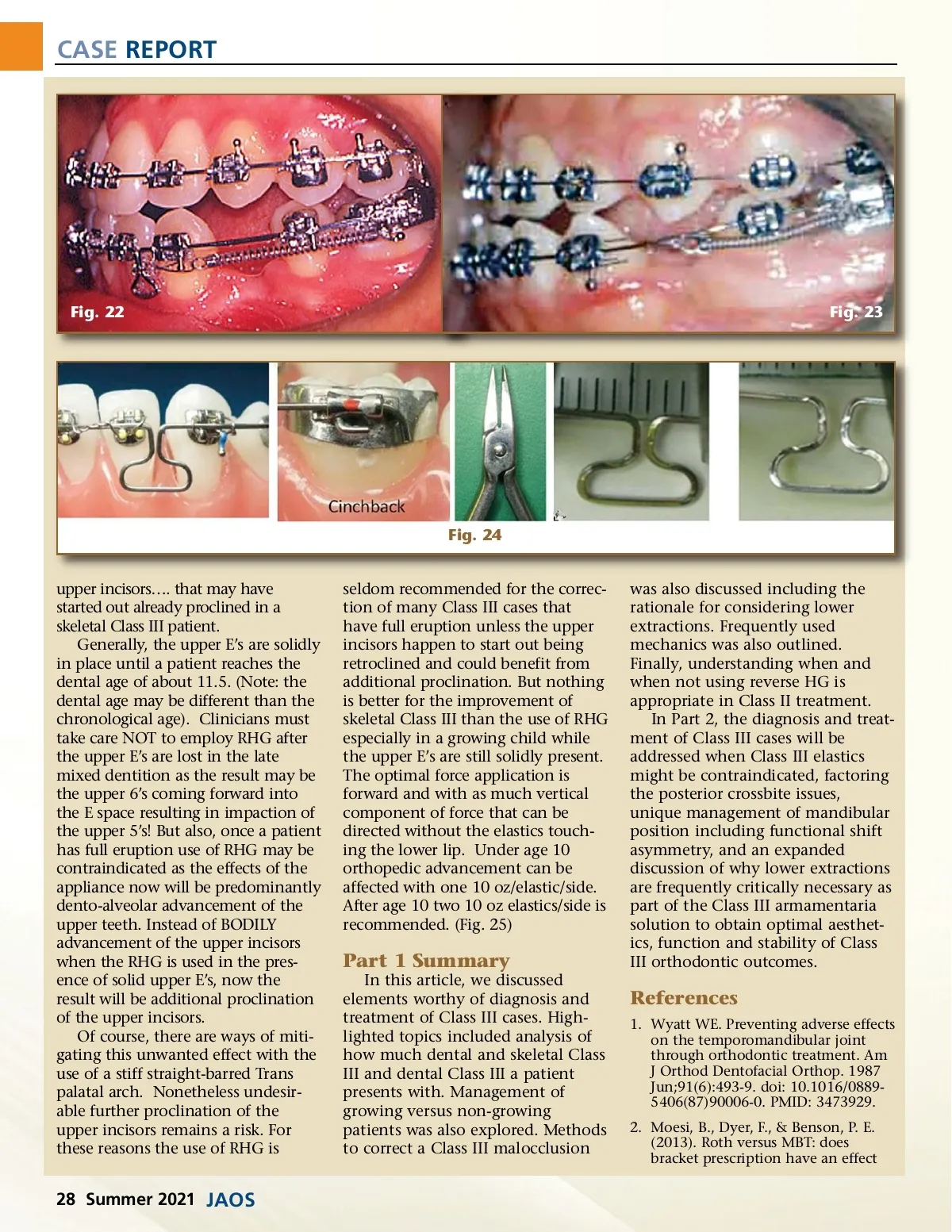
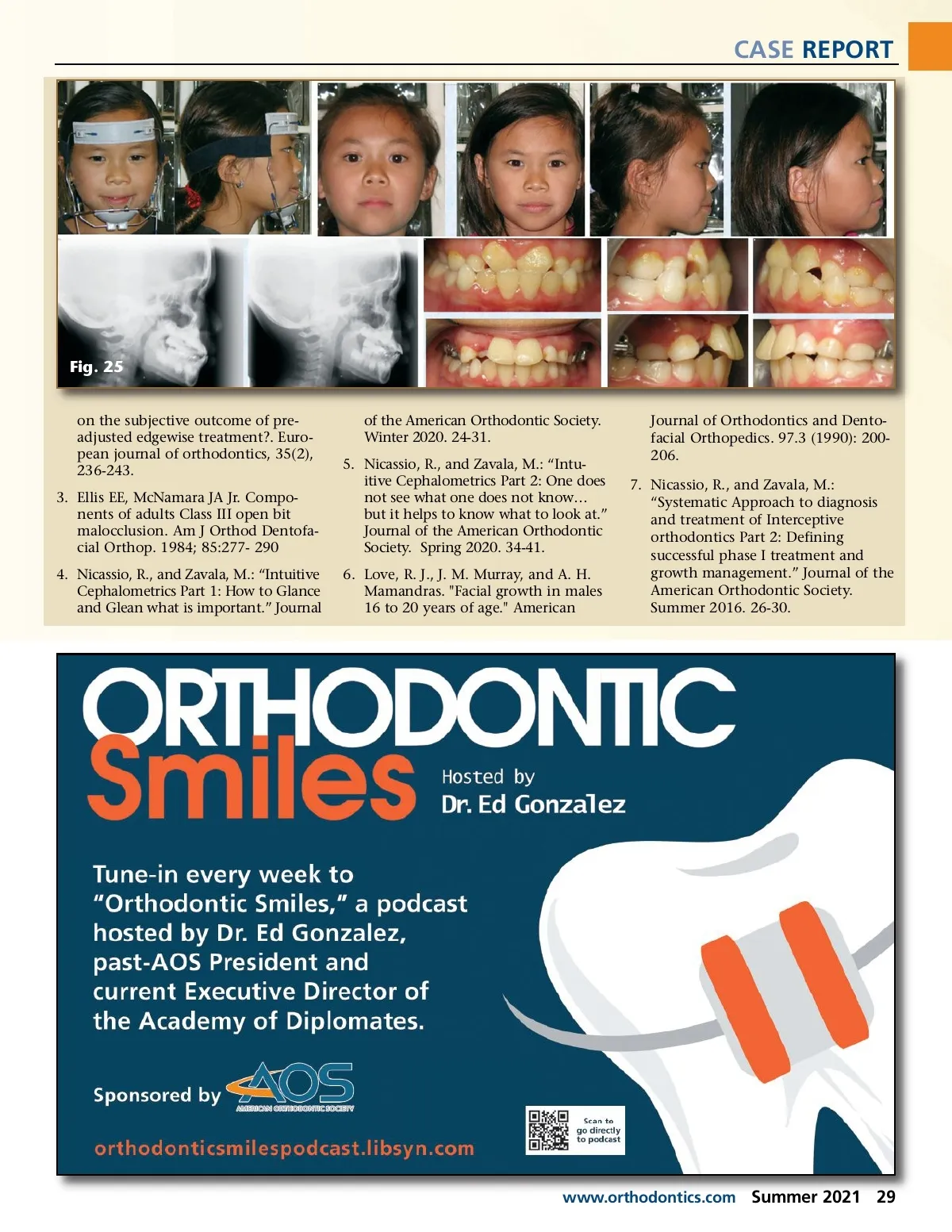
CASE REPORT Fig. 22 Fig. 23 Fig. 24 upper incisors…. that may have started out already proclined in a skeletal Class III patient. Generally, the upper E’s are solidly in place until a patient reaches the dental age of about 11.5. (Note: the dental age may be different than the chronological age). Clinicians must take care NOT to employ RHG after the upper E’s are lost in the late mixed dentition as the result may be the upper 6’s coming forward into the E space resulting in impaction of the upper 5’s! But also, once a patient has full eruption use of RHG may be contraindicated as the effects of the appliance now will be predominantly dento-alveolar advancement of the upper teeth. Instead of BODILY advancement of the upper incisors when the RHG is used in the pres-ence of solid upper E’s, now the result will be additional proclination of the upper incisors. Of course, there are ways of miti-gating this unwanted effect with the use of a stiff straight-barred Trans palatal arch. Nonetheless undesir-able further proclination of the upper incisors remains a risk. For these reasons the use of RHG is seldom recommended for the correc-tion of many Class III cases that have full eruption unless the upper incisors happen to start out being retroclined and could benefit from additional proclination. But nothing is better for the improvement of skeletal Class III than the use of RHG especially in a growing child while the upper E’s are still solidly present. The optimal force application is forward and with as much vertical component of force that can be directed without the elastics touch-ing the lower lip. Under age 10 orthopedic advancement can be affected with one 10 oz/elastic/side. After age 10 two 10 oz elastics/side is recommended. (Fig. 25) was also discussed including the rationale for considering lower extractions. Frequently used mechanics was also outlined. Finally, understanding when and when not using reverse HG is appropriate in Class II treatment. In Part 2, the diagnosis and treat-ment of Class III cases will be addressed when Class III elastics might be contraindicated, factoring the posterior crossbite issues, unique management of mandibular position including functional shift asymmetry, and an expanded discussion of why lower extractions are frequently critically necessary as part of the Class III armamentaria solution to obtain optimal aesthet-ics, function and stability of Class III orthodontic outcomes. Part 1 Summary In this article, we discussed elements worthy of diagnosis and treatment of Class III cases. High-lighted topics included analysis of how much dental and skeletal Class III and dental Class III a patient presents with. Management of growing versus non-growing patients was also explored. Methods to correct a Class III malocclusion References 1. Wyatt WE. Preventing adverse effects on the temporomandibular joint through orthodontic treatment. Am J Orthod Dentofacial Orthop. 1987 Jun;91(6):493-9. doi: 10.1016/0889-5406(87)90006-0. PMID: 3473929. 2. Moesi, B., Dyer, F., & Benson, P. E. (2013). Roth versus MBT: does bracket prescription have an effect 28 Summer 2021 JAOS
Journal of the American Orthodontic Society Summer 2021: Page 28