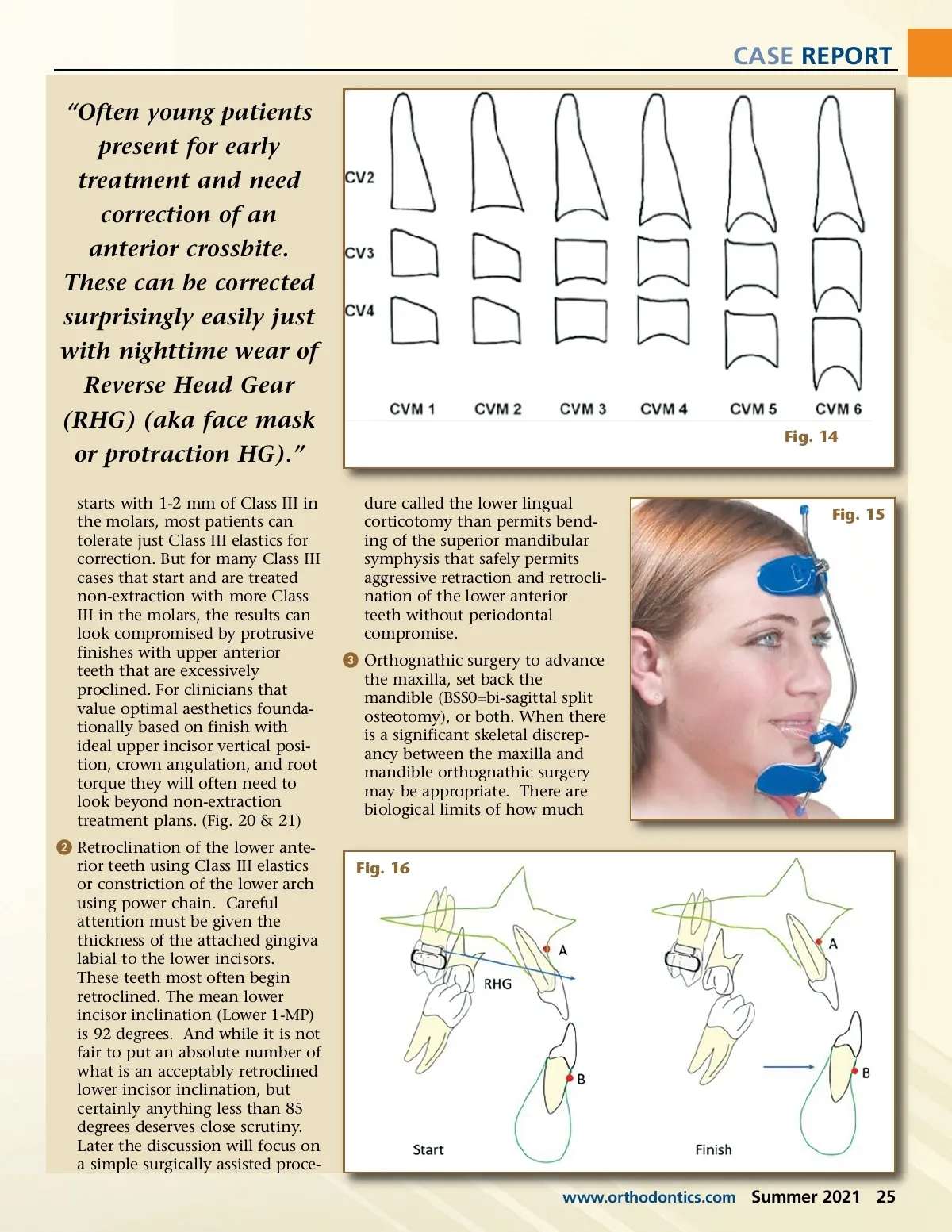
CASE REPORT “Often young patients present for early treatment and need correction of an anterior crossbite. These can be corrected surprisingly easily just with nighttime wear of Reverse Head Gear (RHG) (aka face mask or protraction HG).” starts with 1-2 mm of Class III in the molars, most patients can tolerate just Class III elastics for correction. But for many Class III cases that start and are treated non-extraction with more Class III in the molars, the results can look compromised by protrusive finishes with upper anterior teeth that are excessively proclined. For clinicians that value optimal aesthetics founda-tionally based on finish with ideal upper incisor vertical posi-tion, crown angulation, and root torque they will often need to look beyond non-extraction treatment plans. (Fig. 20 & 21) ᕢ Retroclination of the lower ante-rior teeth using Class III elastics or constriction of the lower arch using power chain. Careful attention must be given the thickness of the attached gingiva labial to the lower incisors. These teeth most often begin retroclined. The mean lower incisor inclination (Lower 1-MP) is 92 degrees. And while it is not fair to put an absolute number of what is an acceptably retroclined lower incisor inclination, but certainly anything less than 85 degrees deserves close scrutiny. Later the discussion will focus on a simple surgically assisted proce-dure called the lower lingual corticotomy than permits bend-ing of the superior mandibular symphysis that safely permits aggressive retraction and retrocli-nation of the lower anterior teeth without periodontal compromise. ᕣ Orthognathic surgery to advance the maxilla, set back the mandible (BSS0=bi-sagittal split osteotomy), or both. When there is a significant skeletal discrep-ancy between the maxilla and mandible orthognathic surgery may be appropriate. There are biological limits of how much Fig. 14 Fig. 15 Fig. 16 www.orthodontics.com Summer 2021 25
Journal of the American Orthodontic Society Summer 2021: Page 25