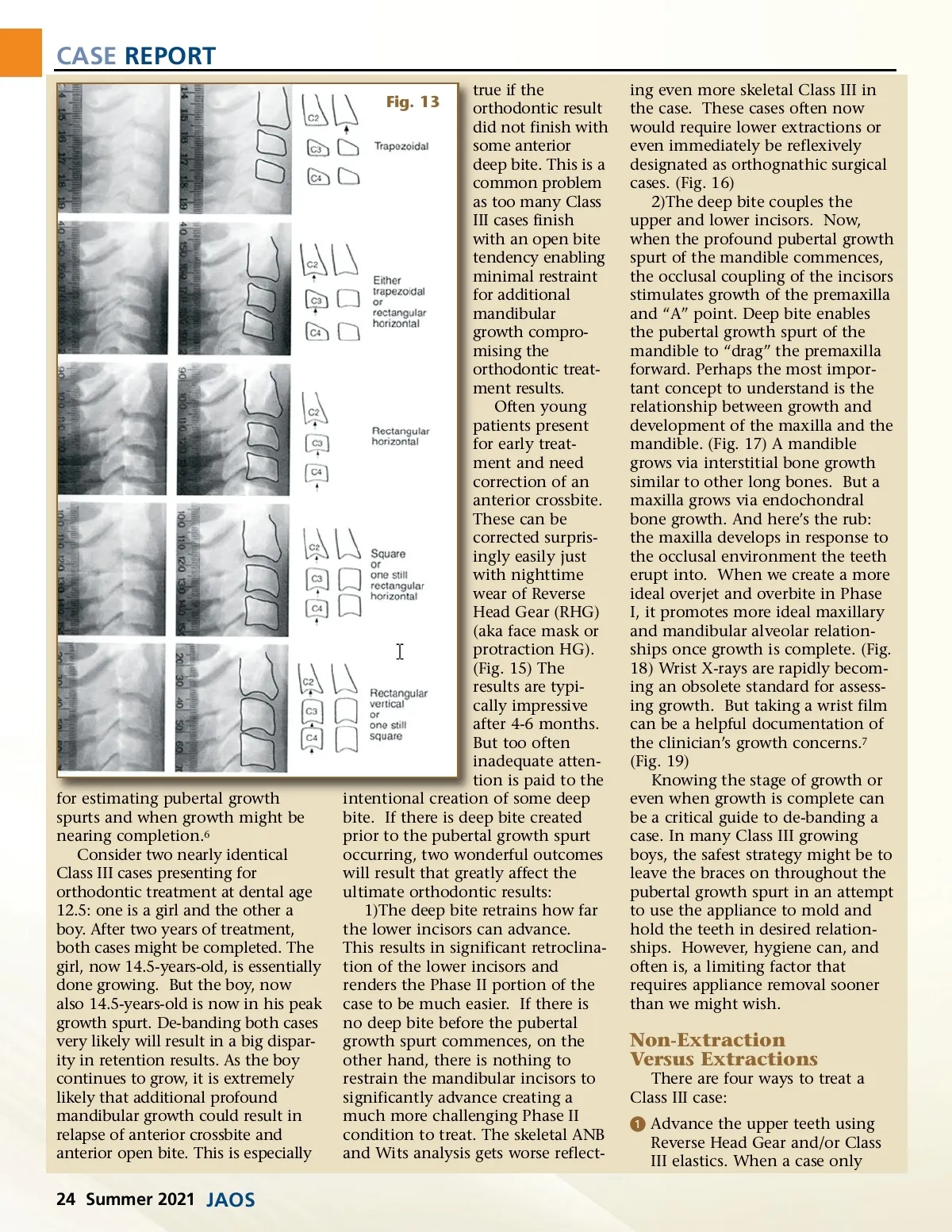
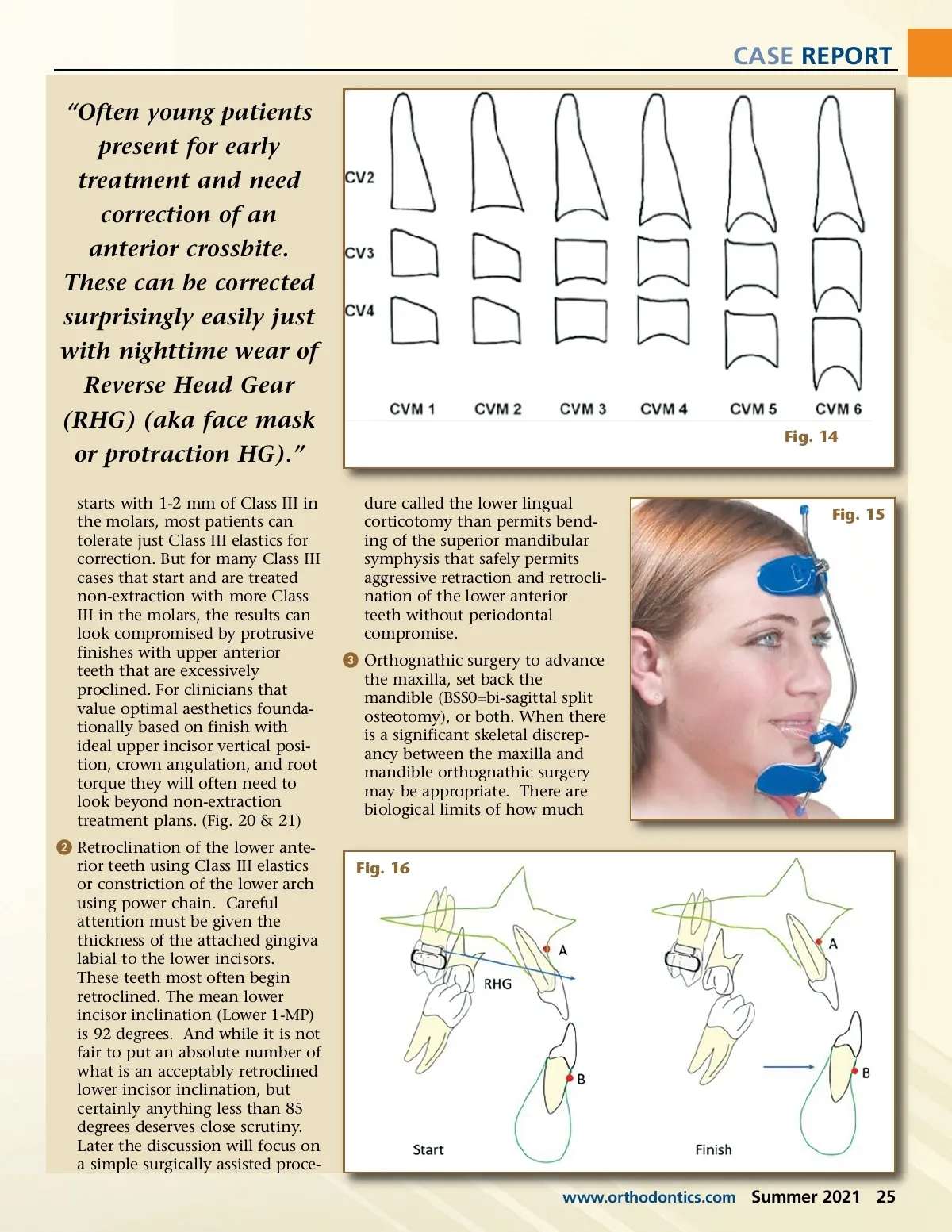
CASE REPORT true if the orthodontic result did not finish with some anterior deep bite. This is a common problem as too many Class III cases finish with an open bite tendency enabling minimal restraint for additional mandibular growth compro-mising the orthodontic treat-ment results. Often young patients present for early treat-ment and need correction of an anterior crossbite. These can be corrected surpris-ingly easily just with nighttime wear of Reverse Head Gear (RHG) (aka face mask or protraction HG). (Fig. 15) The results are typi-cally impressive after 4-6 months. But too often inadequate atten-tion is paid to the intentional creation of some deep bite. If there is deep bite created prior to the pubertal growth spurt occurring, two wonderful outcomes will result that greatly affect the ultimate orthodontic results: 1)The deep bite retrains how far the lower incisors can advance. This results in significant retroclina-tion of the lower incisors and renders the Phase II portion of the case to be much easier. If there is no deep bite before the pubertal growth spurt commences, on the other hand, there is nothing to restrain the mandibular incisors to significantly advance creating a much more challenging Phase II condition to treat. The skeletal ANB and Wits analysis gets worse reflect-Fig. 13 ing even more skeletal Class III in the case. These cases often now would require lower extractions or even immediately be reflexively designated as orthognathic surgical cases. (Fig. 16) 2)The deep bite couples the upper and lower incisors. Now, when the profound pubertal growth spurt of the mandible commences, the occlusal coupling of the incisors stimulates growth of the premaxilla and “A” point. Deep bite enables the pubertal growth spurt of the mandible to “drag” the premaxilla forward. Perhaps the most impor-tant concept to understand is the relationship between growth and development of the maxilla and the mandible. (Fig. 17) A mandible grows via interstitial bone growth similar to other long bones. But a maxilla grows via endochondral bone growth. And here’s the rub: the maxilla develops in response to the occlusal environment the teeth erupt into. When we create a more ideal overjet and overbite in Phase I, it promotes more ideal maxillary and mandibular alveolar relation-ships once growth is complete. (Fig. 18) Wrist X-rays are rapidly becom-ing an obsolete standard for assess-ing growth. But taking a wrist film can be a helpful documentation of the clinician’s growth concerns. 7 (Fig. 19) Knowing the stage of growth or even when growth is complete can be a critical guide to de-banding a case. In many Class III growing boys, the safest strategy might be to leave the braces on throughout the pubertal growth spurt in an attempt to use the appliance to mold and hold the teeth in desired relation-ships. However, hygiene can, and often is, a limiting factor that requires appliance removal sooner than we might wish. for estimating pubertal growth spurts and when growth might be nearing completion. 6 Consider two nearly identical Class III cases presenting for orthodontic treatment at dental age 12.5: one is a girl and the other a boy. After two years of treatment, both cases might be completed. The girl, now 14.5-years-old, is essentially done growing. But the boy, now also 14.5-years-old is now in his peak growth spurt. De-banding both cases very likely will result in a big dispar-ity in retention results. As the boy continues to grow, it is extremely likely that additional profound mandibular growth could result in relapse of anterior crossbite and anterior open bite. This is especially Non-Extraction Versus Extractions There are four ways to treat a Class III case: ᕡ Advance the upper teeth using Reverse Head Gear and/or Class III elastics. When a case only 24 Summer 2021 JAOS
Journal of the American Orthodontic Society Summer 2021: Page 24