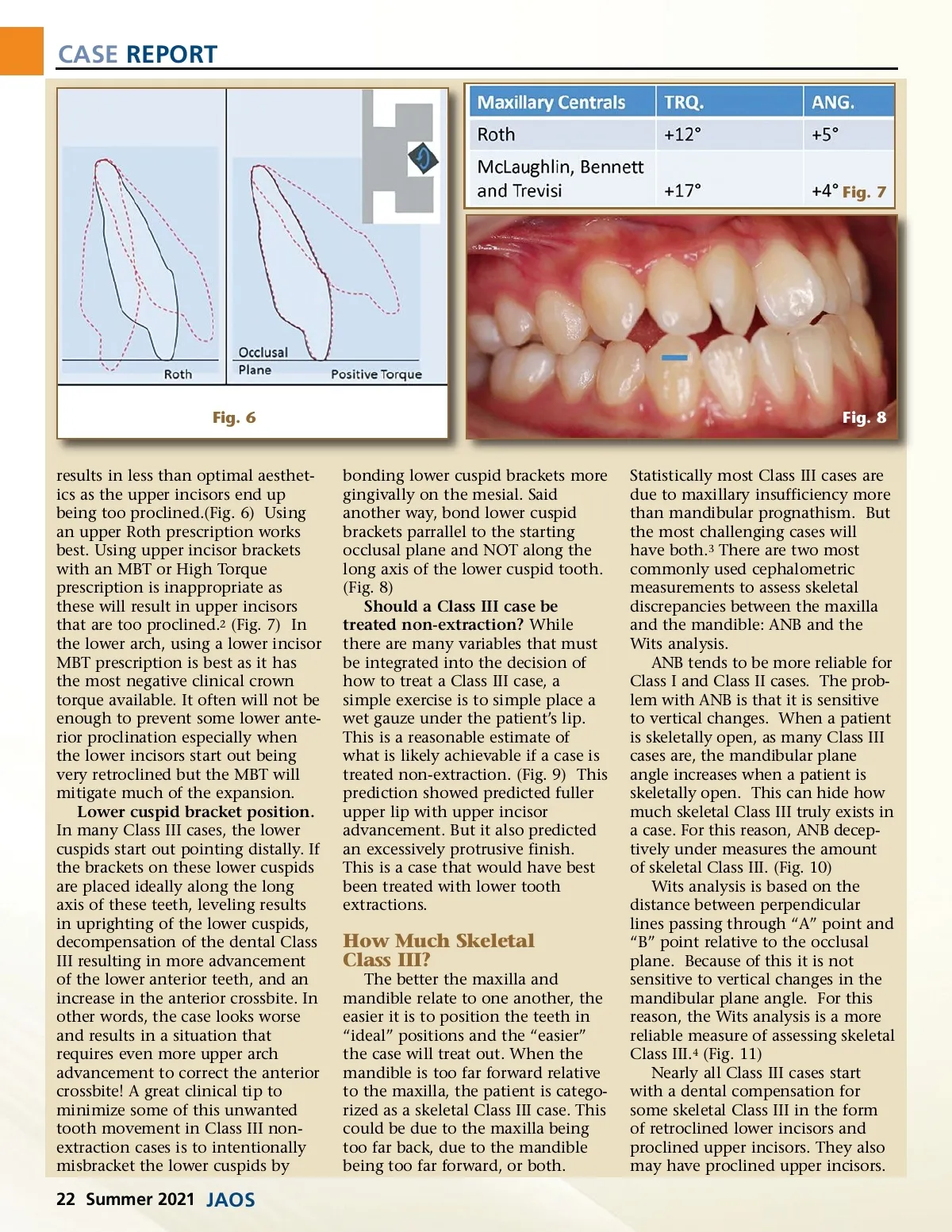
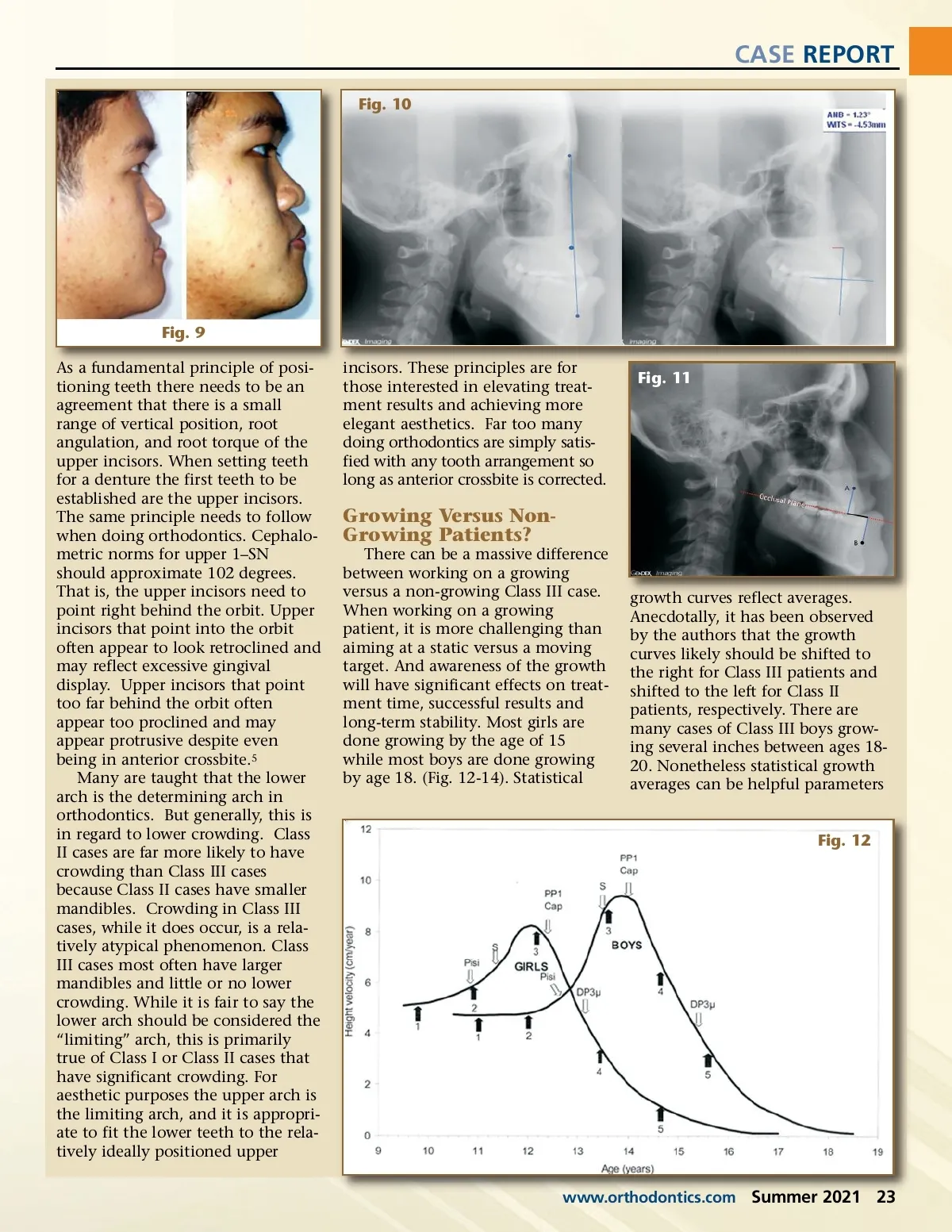
CASE REPORT Fig. 7 Fig. 6 Fig. 8 results in less than optimal aesthet-ics as the upper incisors end up being too proclined.(Fig. 6) Using an upper Roth prescription works best. Using upper incisor brackets with an MBT or High Torque prescription is inappropriate as these will result in upper incisors that are too proclined. 2 (Fig. 7) In the lower arch, using a lower incisor MBT prescription is best as it has the most negative clinical crown torque available. It often will not be enough to prevent some lower ante-rior proclination especially when the lower incisors start out being very retroclined but the MBT will mitigate much of the expansion. Lower cuspid bracket position. In many Class III cases, the lower cuspids start out pointing distally. If the brackets on these lower cuspids are placed ideally along the long axis of these teeth, leveling results in uprighting of the lower cuspids, decompensation of the dental Class III resulting in more advancement of the lower anterior teeth, and an increase in the anterior crossbite. In other words, the case looks worse and results in a situation that requires even more upper arch advancement to correct the anterior crossbite! A great clinical tip to minimize some of this unwanted tooth movement in Class III non-extraction cases is to intentionally misbracket the lower cuspids by bonding lower cuspid brackets more gingivally on the mesial. Said another way, bond lower cuspid brackets parrallel to the starting occlusal plane and NOT along the long axis of the lower cuspid tooth. (Fig. 8) Should a Class III case be treated non-extraction? While there are many variables that must be integrated into the decision of how to treat a Class III case, a simple exercise is to simple place a wet gauze under the patient’s lip. This is a reasonable estimate of what is likely achievable if a case is treated non-extraction. (Fig. 9) This prediction showed predicted fuller upper lip with upper incisor advancement. But it also predicted an excessively protrusive finish. This is a case that would have best been treated with lower tooth extractions. How Much Skeletal Class III? The better the maxilla and mandible relate to one another, the easier it is to position the teeth in “ideal” positions and the “easier” the case will treat out. When the mandible is too far forward relative to the maxilla, the patient is catego-rized as a skeletal Class III case. This could be due to the maxilla being too far back, due to the mandible being too far forward, or both. Statistically most Class III cases are due to maxillary insufficiency more than mandibular prognathism. But the most challenging cases will have both. 3 There are two most commonly used cephalometric measurements to assess skeletal discrepancies between the maxilla and the mandible: ANB and the Wits analysis. ANB tends to be more reliable for Class I and Class II cases. The prob-lem with ANB is that it is sensitive to vertical changes. When a patient is skeletally open, as many Class III cases are, the mandibular plane angle increases when a patient is skeletally open. This can hide how much skeletal Class III truly exists in a case. For this reason, ANB decep-tively under measures the amount of skeletal Class III. (Fig. 10) Wits analysis is based on the distance between perpendicular lines passing through “A” point and “B” point relative to the occlusal plane. Because of this it is not sensitive to vertical changes in the mandibular plane angle. For this reason, the Wits analysis is a more reliable measure of assessing skeletal Class III. 4 (Fig. 11) Nearly all Class III cases start with a dental compensation for some skeletal Class III in the form of retroclined lower incisors and proclined upper incisors. They also may have proclined upper incisors. 22 Summer 2021 JAOS
Journal of the American Orthodontic Society Summer 2021: Page 22