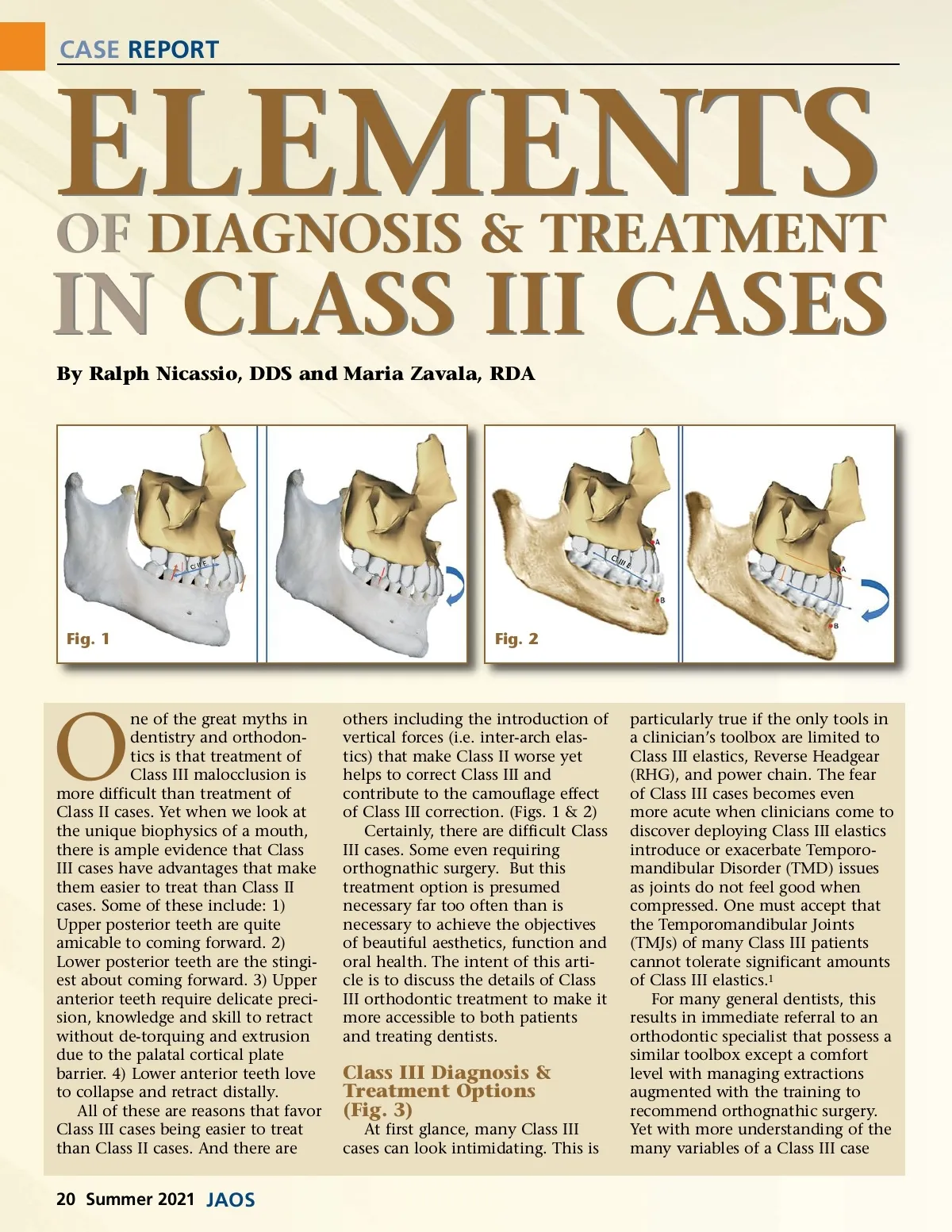
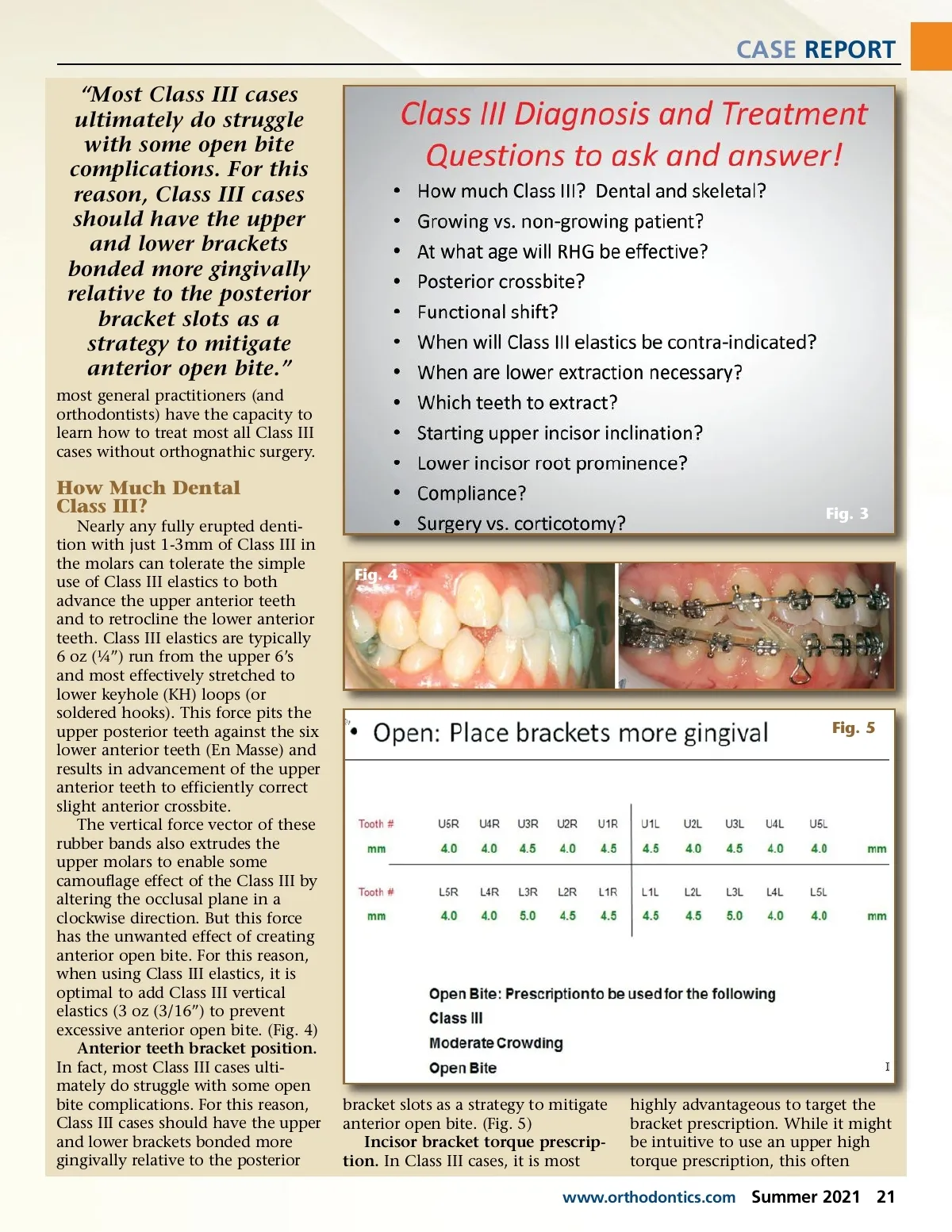
CASE REPORT “Most Class III cases ultimately do struggle with some open bite complications. For this reason, Class III cases should have the upper and lower brackets bonded more gingivally relative to the posterior bracket slots as a strategy to mitigate anterior open bite.” most general practitioners (and orthodontists) have the capacity to learn how to treat most all Class III cases without orthognathic surgery. How Much Dental Class III? Nearly any fully erupted denti-tion with just 1-3mm of Class III in the molars can tolerate the simple use of Class III elastics to both advance the upper anterior teeth and to retrocline the lower anterior teeth. Class III elastics are typically 6 oz (¼”) run from the upper 6’s and most effectively stretched to lower keyhole (KH) loops (or soldered hooks). This force pits the upper posterior teeth against the six lower anterior teeth (En Masse) and results in advancement of the upper anterior teeth to efficiently correct slight anterior crossbite. The vertical force vector of these rubber bands also extrudes the upper molars to enable some camouflage effect of the Class III by altering the occlusal plane in a clockwise direction. But this force has the unwanted effect of creating anterior open bite. For this reason, when using Class III elastics, it is optimal to add Class III vertical elastics (3 oz (3/16”) to prevent excessive anterior open bite. (Fig. 4) Anterior teeth bracket position. In fact, most Class III cases ulti-mately do struggle with some open bite complications. For this reason, Class III cases should have the upper and lower brackets bonded more gingivally relative to the posterior Fig. 3 Fig. 4 Fig. 5 bracket slots as a strategy to mitigate anterior open bite. (Fig. 5) Incisor bracket torque prescrip-tion. In Class III cases, it is most highly advantageous to target the bracket prescription. While it might be intuitive to use an upper high torque prescription, this often www.orthodontics.com Summer 2021 21
Journal of the American Orthodontic Society Summer 2021: Page 21