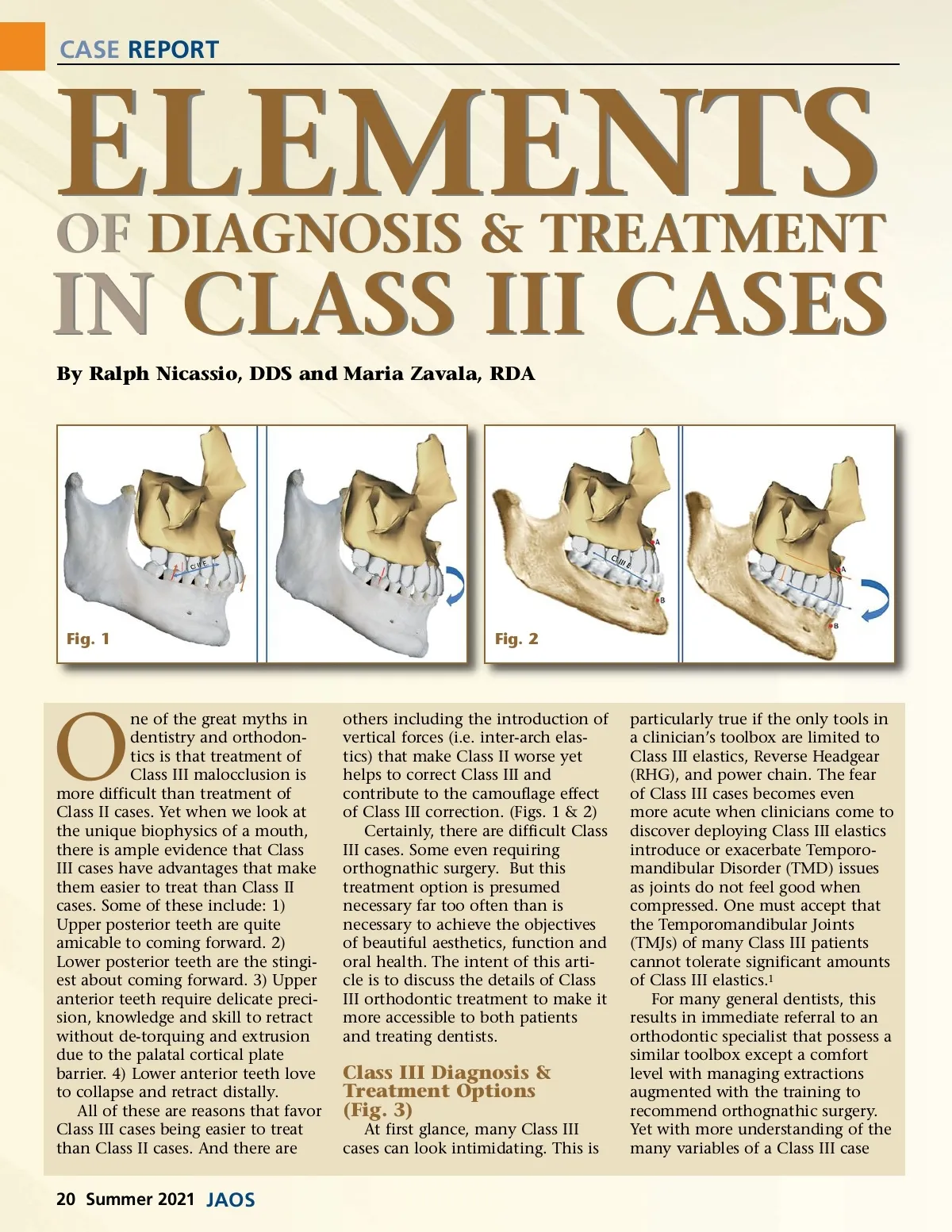
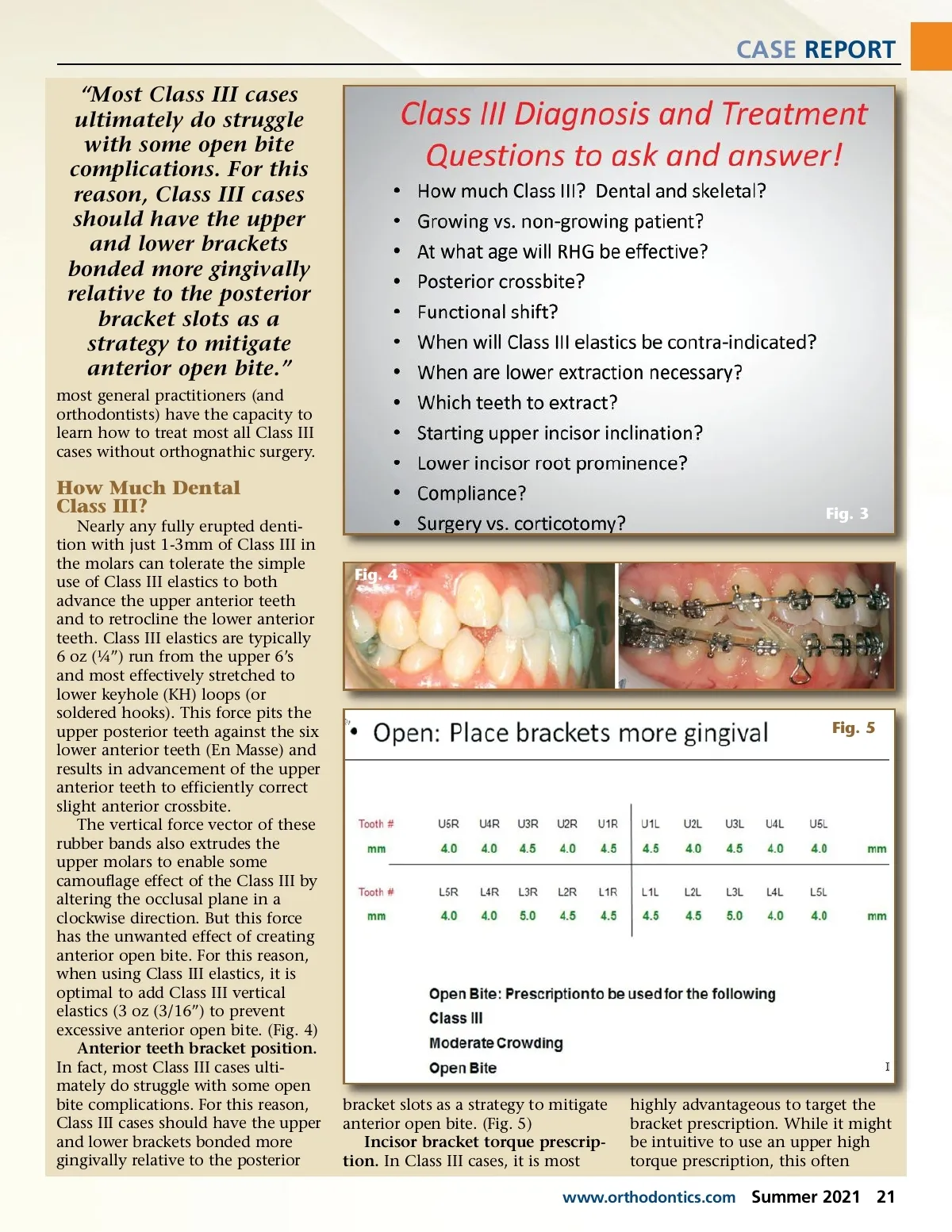
CASE REPORT ELEMENTS By Ralph Nicassio, DDS and Maria Zavala, RDA OF DIAGNOSIS & TREATMENT IN CLASS III CASES Fig. 1 Fig. 2 O ne of the great myths in dentistry and orthodon-tics is that treatment of Class III malocclusion is more difficult than treatment of Class II cases. Yet when we look at the unique biophysics of a mouth, there is ample evidence that Class III cases have advantages that make them easier to treat than Class II cases. Some of these include: 1) Upper posterior teeth are quite amicable to coming forward. 2) Lower posterior teeth are the stingi-est about coming forward. 3) Upper anterior teeth require delicate preci-sion, knowledge and skill to retract without de-torquing and extrusion due to the palatal cortical plate barrier. 4) Lower anterior teeth love to collapse and retract distally. All of these are reasons that favor Class III cases being easier to treat than Class II cases. And there are others including the introduction of vertical forces (i.e. inter-arch elas-tics) that make Class II worse yet helps to correct Class III and contribute to the camouflage effect of Class III correction. (Figs. 1 & 2) Certainly, there are difficult Class III cases. Some even requiring orthognathic surgery. But this treatment option is presumed necessary far too often than is necessary to achieve the objectives of beautiful aesthetics, function and oral health. The intent of this arti-cle is to discuss the details of Class III orthodontic treatment to make it more accessible to both patients and treating dentists. Class III Diagnosis & Treatment Options (Fig. 3) At first glance, many Class III cases can look intimidating. This is particularly true if the only tools in a clinician’s toolbox are limited to Class III elastics, Reverse Headgear (RHG), and power chain. The fear of Class III cases becomes even more acute when clinicians come to discover deploying Class III elastics introduce or exacerbate Temporo-mandibular Disorder (TMD) issues as joints do not feel good when compressed. One must accept that the Temporomandibular Joints (TMJs) of many Class III patients cannot tolerate significant amounts of Class III elastics. 1 For many general dentists, this results in immediate referral to an orthodontic specialist that possess a similar toolbox except a comfort level with managing extractions augmented with the training to recommend orthognathic surgery. Yet with more understanding of the many variables of a Class III case 20 Summer 2021 JAOS
Journal of the American Orthodontic Society Summer 2021: Page 20