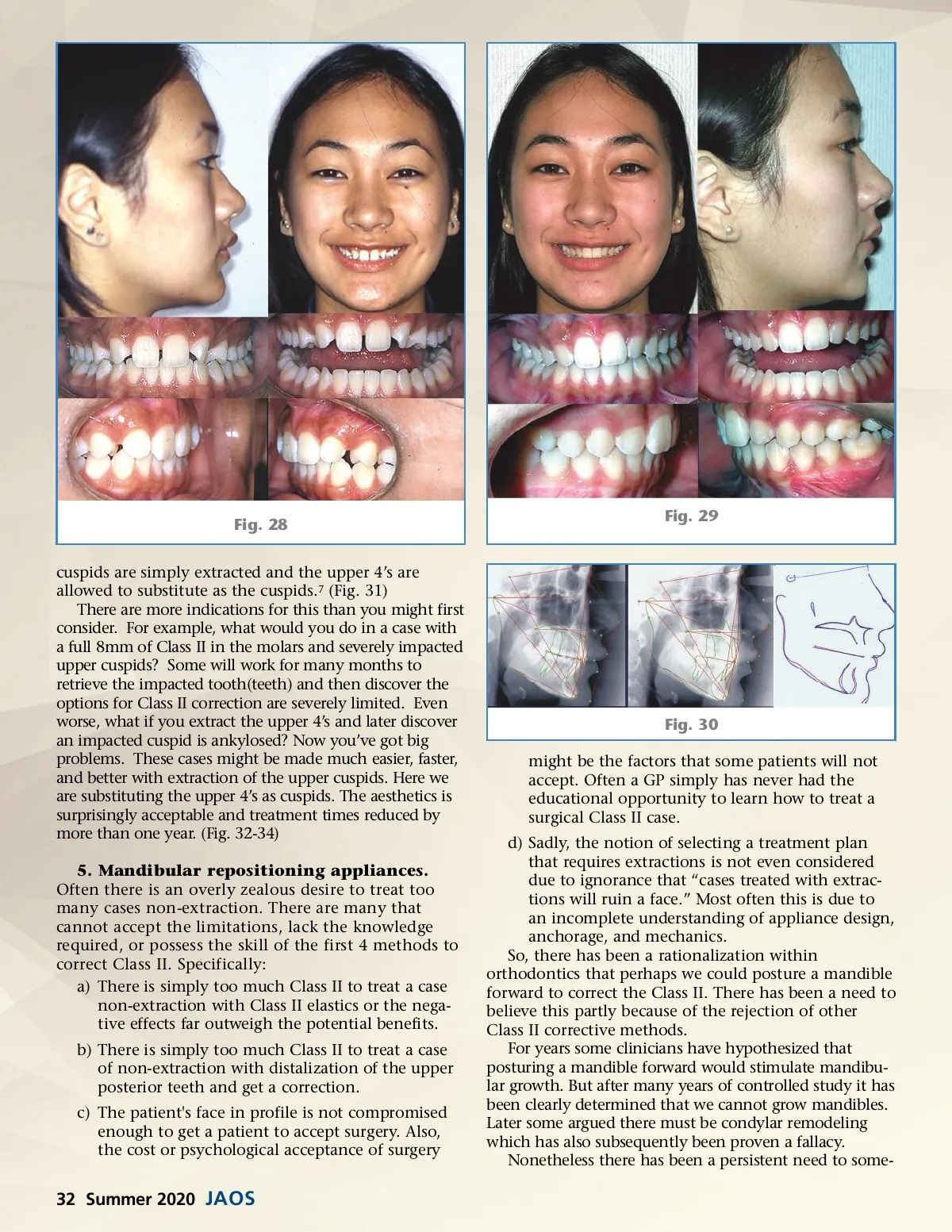
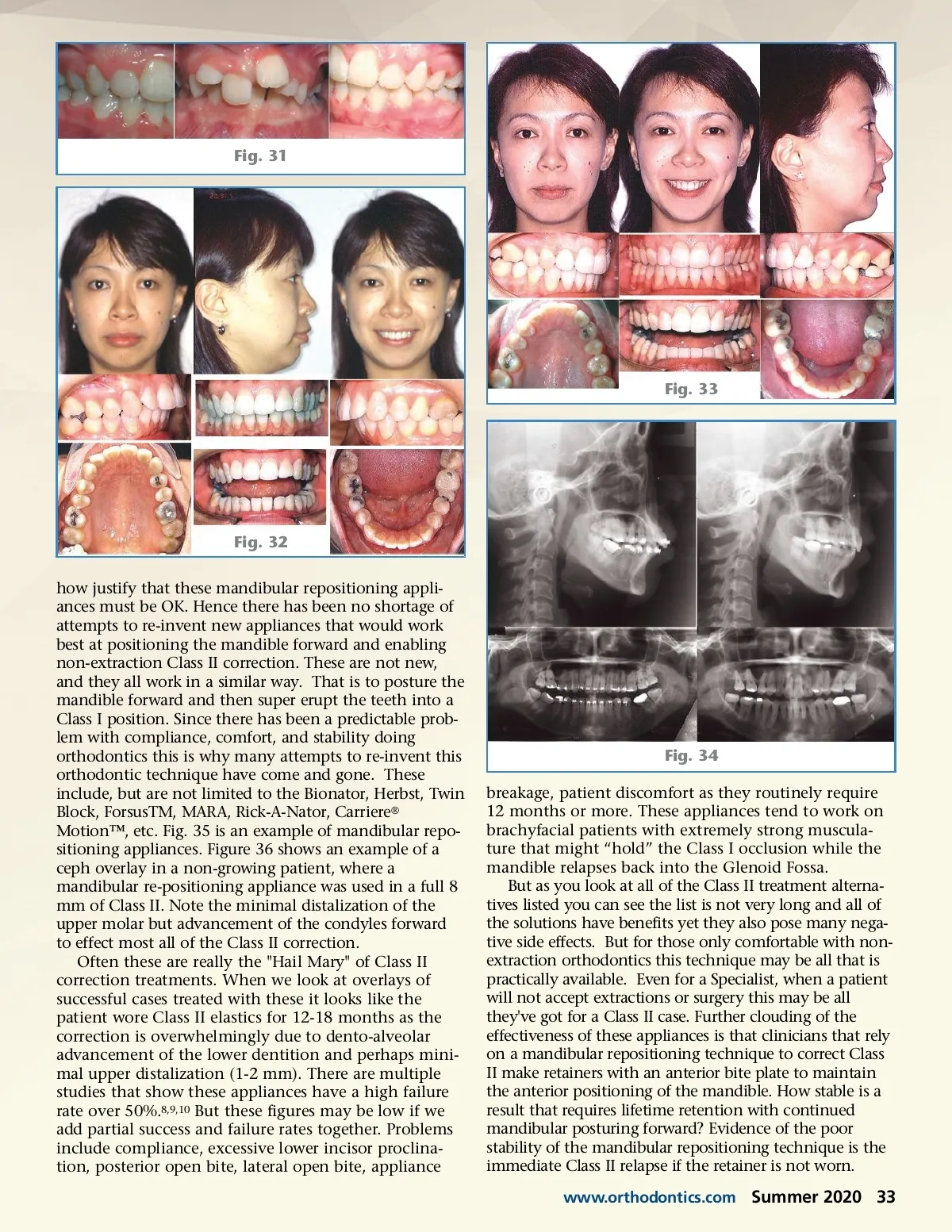
Fig. 31 Fig. 33 Fig. 32 how justify that these mandibular repositioning appli-ances must be OK. Hence there has been no shortage of attempts to re-invent new appliances that would work best at positioning the mandible forward and enabling non-extraction Class II correction. These are not new, and they all work in a similar way. That is to posture the mandible forward and then super erupt the teeth into a Class I position. Since there has been a predictable prob-lem with compliance, comfort, and stability doing orthodontics this is why many attempts to re-invent this orthodontic technique have come and gone. These include, but are not limited to the Bionator, Herbst, Twin Block, ForsusTM, MARA, Rick-A-Nator, Carriere ® Motion™, etc. Fig. 35 is an example of mandibular repo-sitioning appliances. Figure 36 shows an example of a ceph overlay in a non-growing patient, where a mandibular re-positioning appliance was used in a full 8 mm of Class II. Note the minimal distalization of the upper molar but advancement of the condyles forward to effect most all of the Class II correction. Often these are really the "Hail Mary" of Class II correction treatments. When we look at overlays of successful cases treated with these it looks like the patient wore Class II elastics for 12-18 months as the correction is overwhelmingly due to dento-alveolar advancement of the lower dentition and perhaps mini-mal upper distalization (1-2 mm). There are multiple studies that show these appliances have a high failure rate over 50%. 8,9,10 But these figures may be low if we add partial success and failure rates together. Problems include compliance, excessive lower incisor proclina-tion, posterior open bite, lateral open bite, appliance Fig. 34 breakage, patient discomfort as they routinely require 12 months or more. These appliances tend to work on brachyfacial patients with extremely strong muscula-ture that might “hold” the Class I occlusion while the mandible relapses back into the Glenoid Fossa. But as you look at all of the Class II treatment alterna-tives listed you can see the list is not very long and all of the solutions have benefits yet they also pose many nega-tive side effects. But for those only comfortable with non-extraction orthodontics this technique may be all that is practically available. Even for a Specialist, when a patient will not accept extractions or surgery this may be all they've got for a Class II case. Further clouding of the effectiveness of these appliances is that clinicians that rely on a mandibular repositioning technique to correct Class II make retainers with an anterior bite plate to maintain the anterior positioning of the mandible. How stable is a result that requires lifetime retention with continued mandibular posturing forward? Evidence of the poor stability of the mandibular repositioning technique is the immediate Class II relapse if the retainer is not worn. www.orthodontics.com Summer 2020 33
Journal of the American Orthodontic Society Summer 2020: Page 33