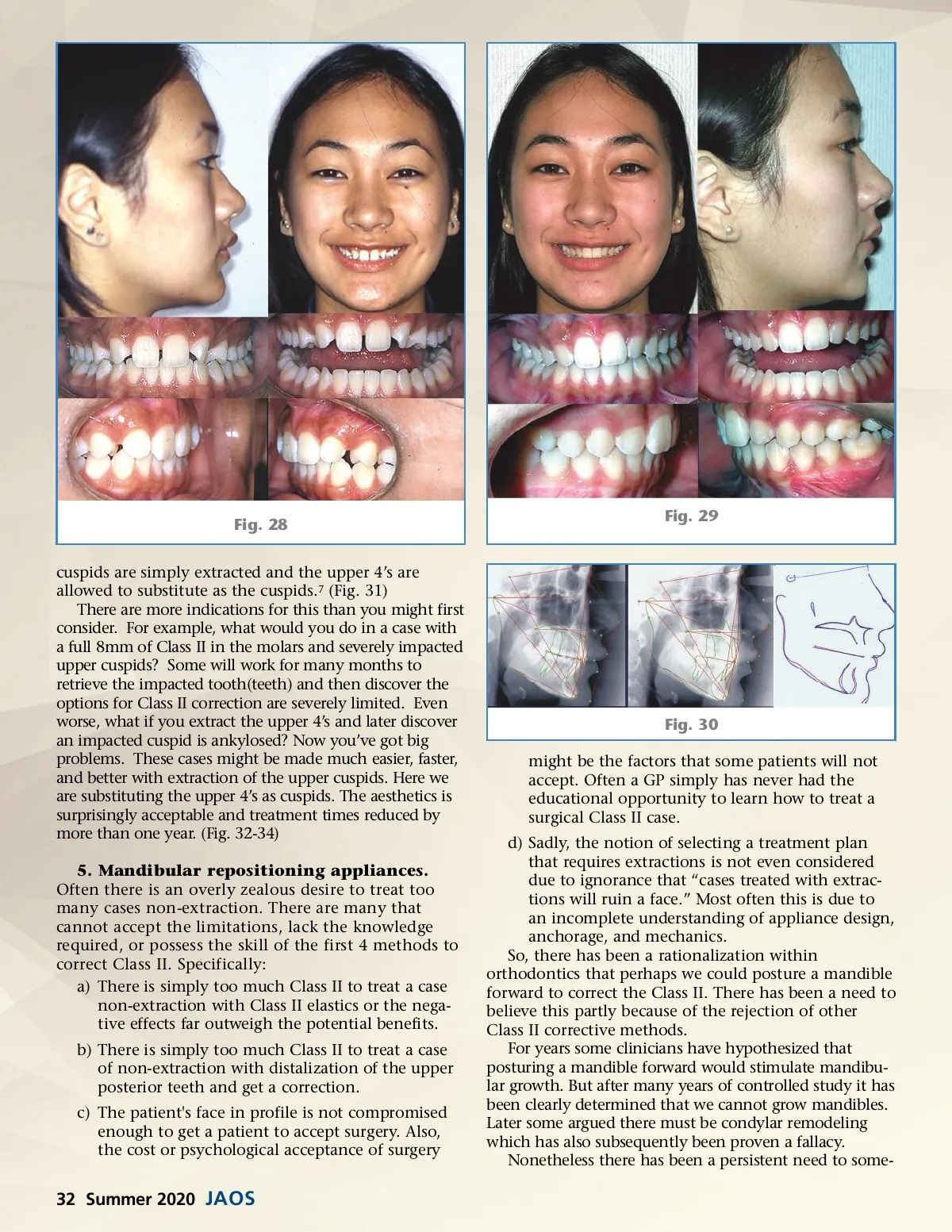
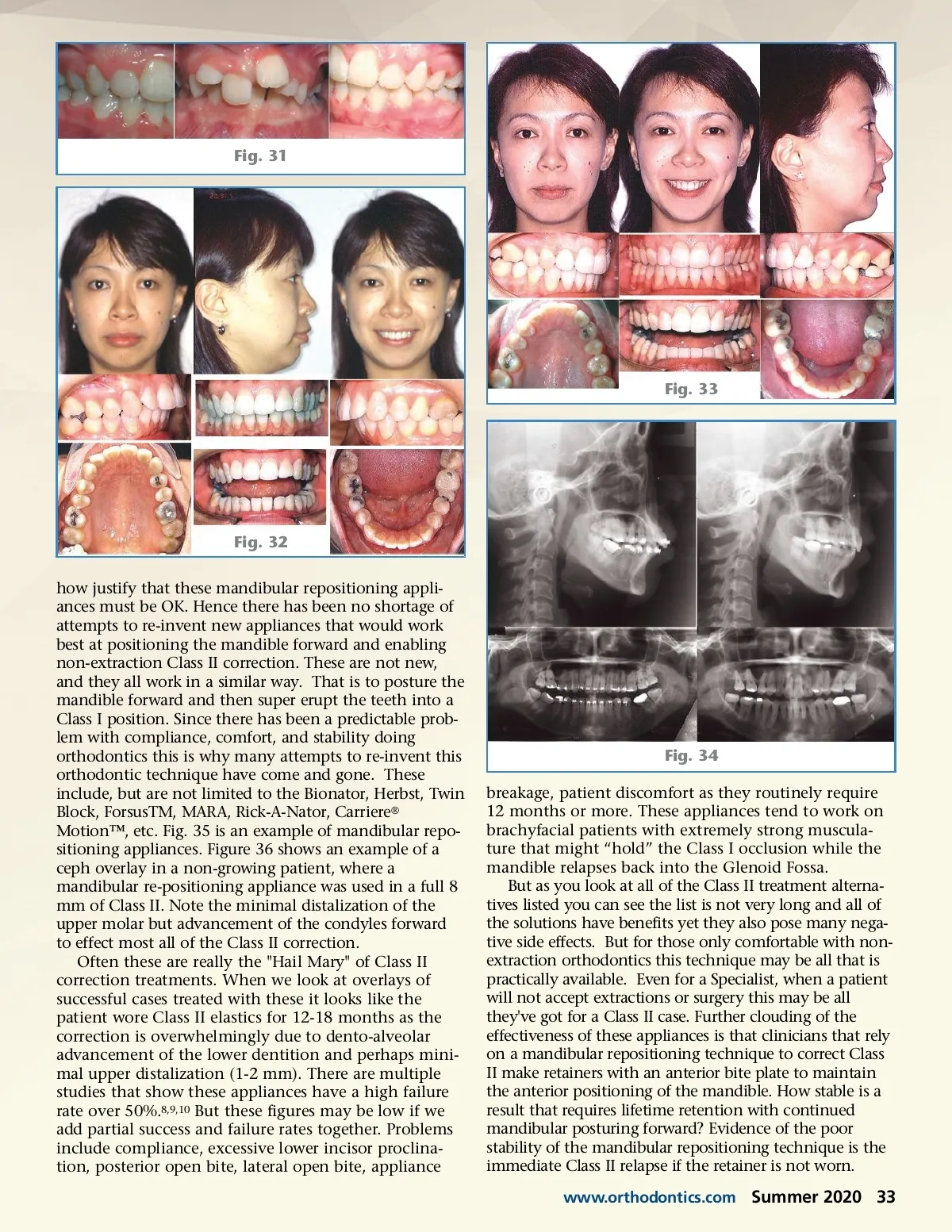
Fig. 28 cuspids are simply extracted and the upper 4’s are allowed to substitute as the cuspids. 7 (Fig. 31) There are more indications for this than you might first consider. For example, what would you do in a case with a full 8mm of Class II in the molars and severely impacted upper cuspids? Some will work for many months to retrieve the impacted tooth(teeth) and then discover the options for Class II correction are severely limited. Even worse, what if you extract the upper 4’s and later discover an impacted cuspid is ankylosed? Now you’ve got big problems. These cases might be made much easier, faster, and better with extraction of the upper cuspids. Here we are substituting the upper 4’s as cuspids. The aesthetics is surprisingly acceptable and treatment times reduced by more than one year. (Fig. 32-34) 5. Mandibular repositioning appliances. Often there is an overly zealous desire to treat too many cases non-extraction. There are many that cannot accept the limitations, lack the knowledge required, or possess the skill of the first 4 methods to correct Class II. Specifically: a) There is simply too much Class II to treat a case non-extraction with Class II elastics or the nega-tive effects far outweigh the potential benefits. b) There is simply too much Class II to treat a case of non-extraction with distalization of the upper posterior teeth and get a correction. c) The patient's face in profile is not compromised enough to get a patient to accept surgery. Also, the cost or psychological acceptance of surgery Fig. 29 Fig. 30 might be the factors that some patients will not accept. Often a GP simply has never had the educational opportunity to learn how to treat a surgical Class II case. d) Sadly, the notion of selecting a treatment plan that requires extractions is not even considered due to ignorance that “cases treated with extrac-tions will ruin a face.” Most often this is due to an incomplete understanding of appliance design, anchorage, and mechanics. So, there has been a rationalization within orthodontics that perhaps we could posture a mandible forward to correct the Class II. There has been a need to believe this partly because of the rejection of other Class II corrective methods. For years some clinicians have hypothesized that posturing a mandible forward would stimulate mandibu-lar growth. But after many years of controlled study it has been clearly determined that we cannot grow mandibles. Later some argued there must be condylar remodeling which has also subsequently been proven a fallacy. Nonetheless there has been a persistent need to some-32 Summer 2020 JAOS
Journal of the American Orthodontic Society Summer 2020: Page 32