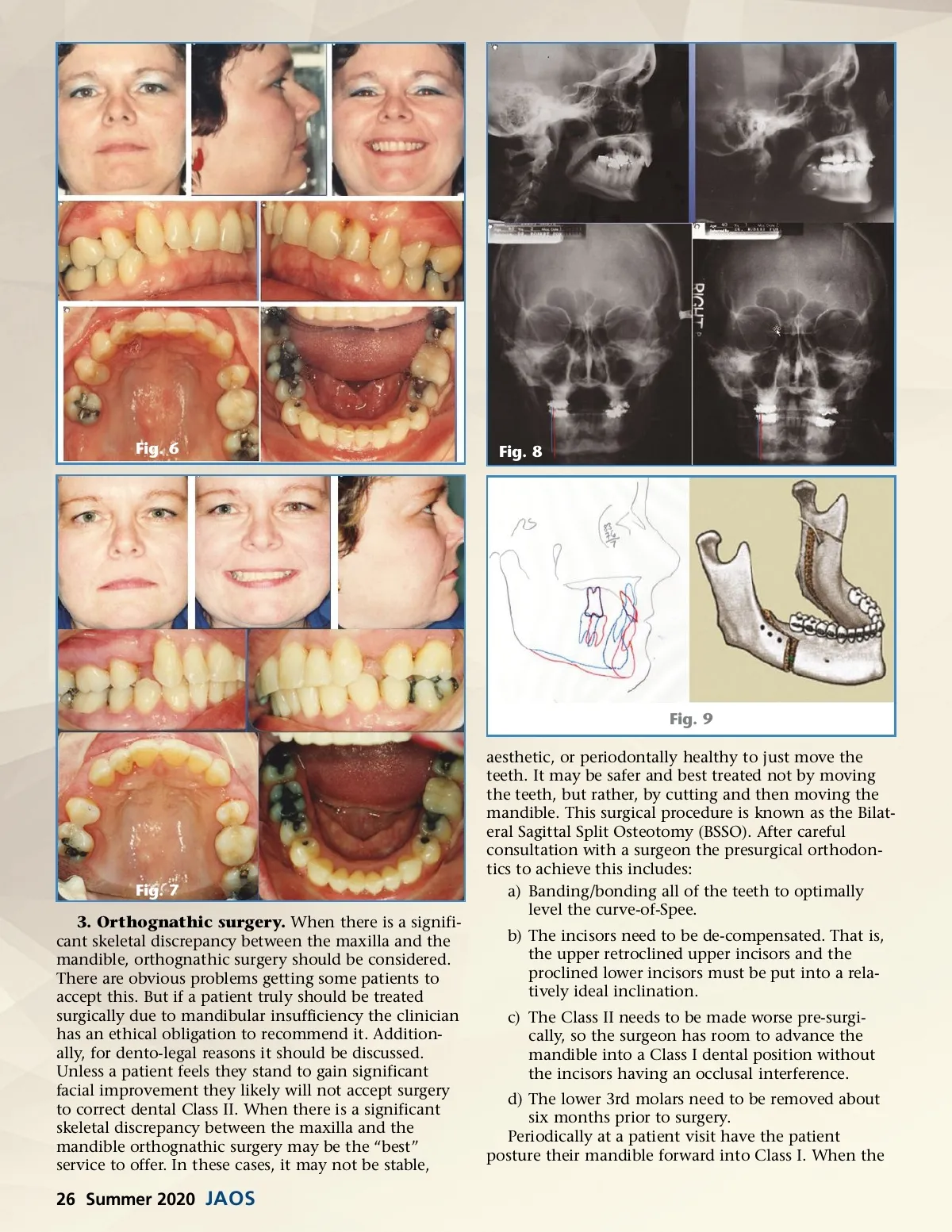
Fig. 11 Fig. 10 teeth fit together, they are ready for surgery. If the teeth cannot be fitted together into Class I posturally, it is possible two-jaw surgeries might be required. In addition to the mandibular advancement these cases might need either a reduction or augmentation genioplasty to optimize profile aesthetics. The following example shows a case that should have been treated surgically but, instead, was treated with extraction of the upper 4’s.(Figs. 6-9) The poor result left the upper incisors periodontally compro-mised. Reopening the upper four spaces and a mandibular advancement was ultimately needed to improve her dental prognosis. It is critically important to note from the lateral and frontal cephalometric films that the only way to increase a patient’s skeletal vertical dimension of occlusion is with orthognathic surgery. Many patients that have a failing dentition will also have a failed restorative future unless orthognathic surgery is the treatment alternative selected to alter the facial musculature and skeletal relationship. 4.a) Extraction of upper bicuspids (4's or 5's). In the 1970’s many Orthodontists began the Class II treatment plan of extracting two upper bicuspids. Until then dental classifications were always based on the molar relationship. But when just two upper bicuspids were extracted it became acceptable to maintain the Class II molar relationship at the expense of getting the cuspids into Class I. Hence the expression, “Molar is King” was born and this treatment alternative coined camouflage Class II correction. This is often the best plan when there are no upper 3rd molars, when the upper 3rd molars are small anatomically, or when the maxillary sinus is low. It may also be appropriate in many adults that want shorter treatment times. There must be recognition that the smile width is compro-mised when this is done. Although this is often appro-Fig. 12 priate it is definitely the most over-diagnosed treatment plan for correction of Class II. It should be noted there are severe Class II cases where extraction of just two upper bicuspids does not create enough space for complete Class II correction.(Fig. 10) Also, there are cases where the upper 5’s are damaged, congenitally missing, small anatomically, or less aesthetic than the upper 4’s. In these situations, extraction of the upper 5’s might be the best service to the patient. (Fig. 11). An advantage of this plan is the mandible is allowed to remain in its original and stable position. Often these cases do not require patient compliance. Mechanics entails maximum upper posterior anchor-age, full retraction of the cuspids into the upper 4 extraction site, then frictionless closing loop retraction of the upper incisors best done with 19x25 reverse curve T-loops (Ormco). (Fig. 12), And as previously mentioned, upper incisors should have a High Torque bracket prescription when they need to be retracted. The challenge with this plan is to retract the upper anterior and maintain ideal aesthetic crown torque. 4.b) Four bicuspid extraction. In any case where lower teeth need to be removed Class II correc-tion is particularly difficult. The reason is the most difficult to move in any patient's mouth are the lower 6's. These teeth are very reluctant to move forward. In general, it is a bad idea to extract teeth in any Class II case as we need to preserve as much lower tooth mass as possible. Any Class II case that requires lower extrac-tions will be a challenging case and should be handled with great care. The reason why it may be appropriate to extract four bicuspids is to create space to retract the upper cuspids into Class I, and advance the lower molars into Class I, without excessively advancing the lower incisors. If the decision has been made to extract www.orthodontics.com Summer 2020 27
Journal of the American Orthodontic Society Summer 2020: Page 27