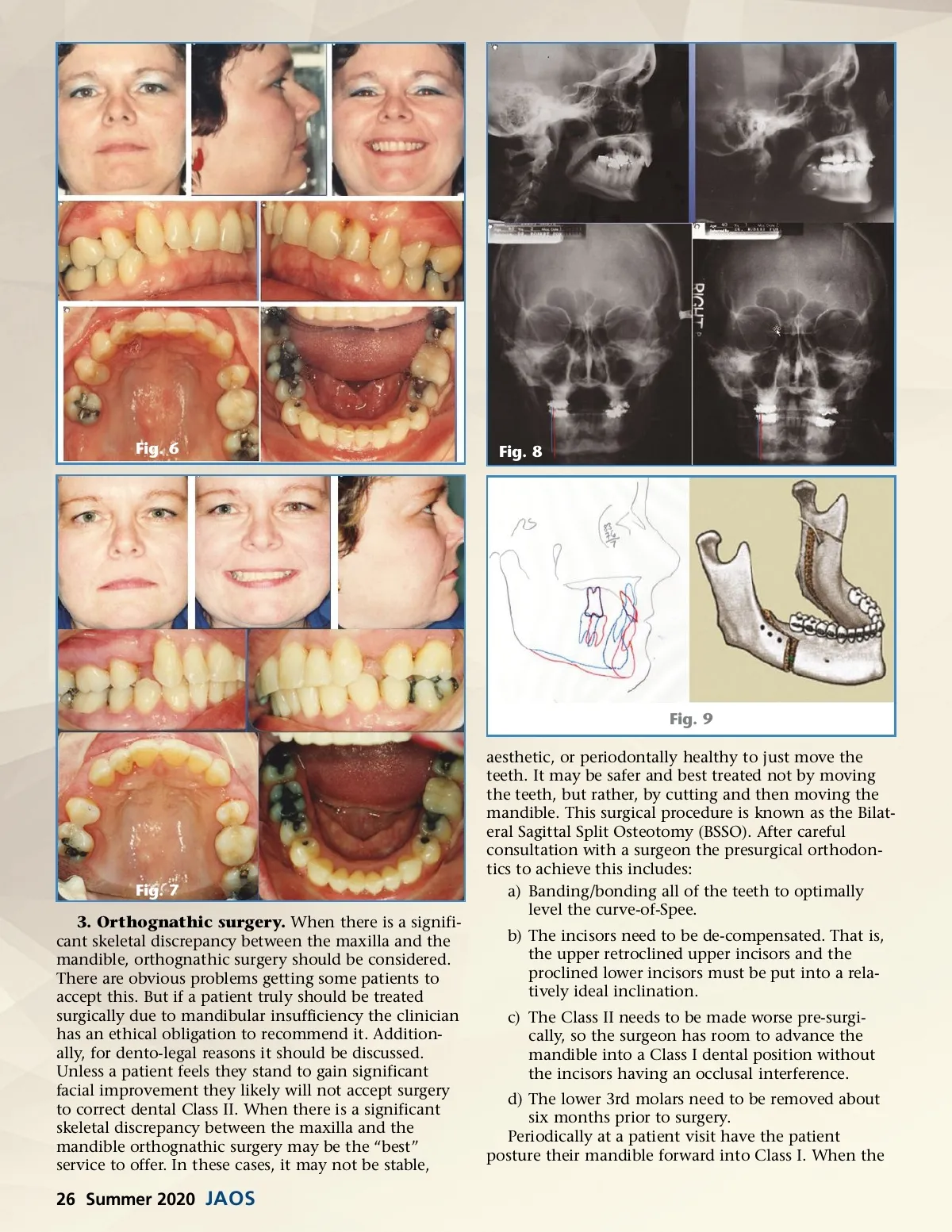
Fig. 6 Fig. 8 Fig. 9 aesthetic, or periodontally healthy to just move the teeth. It may be safer and best treated not by moving the teeth, but rather, by cutting and then moving the mandible. This surgical procedure is known as the Bilat-eral Sagittal Split Osteotomy (BSSO). After careful consultation with a surgeon the presurgical orthodon-tics to achieve this includes: a) Banding/bonding all of the teeth to optimally level the curve-of-Spee. b) The incisors need to be de-compensated. That is, the upper retroclined upper incisors and the proclined lower incisors must be put into a rela-tively ideal inclination. c) The Class II needs to be made worse pre-surgi-cally, so the surgeon has room to advance the mandible into a Class I dental position without the incisors having an occlusal interference. d) The lower 3rd molars need to be removed about six months prior to surgery. Periodically at a patient visit have the patient posture their mandible forward into Class I. When the Fig. 7 3. Orthognathic surgery. When there is a signifi-cant skeletal discrepancy between the maxilla and the mandible, orthognathic surgery should be considered. There are obvious problems getting some patients to accept this. But if a patient truly should be treated surgically due to mandibular insufficiency the clinician has an ethical obligation to recommend it. Addition-ally, for dento-legal reasons it should be discussed. Unless a patient feels they stand to gain significant facial improvement they likely will not accept surgery to correct dental Class II. When there is a significant skeletal discrepancy between the maxilla and the mandible orthognathic surgery may be the “best” service to offer. In these cases, it may not be stable, 26 Summer 2020 JAOS
Journal of the American Orthodontic Society Summer 2020: Page 26