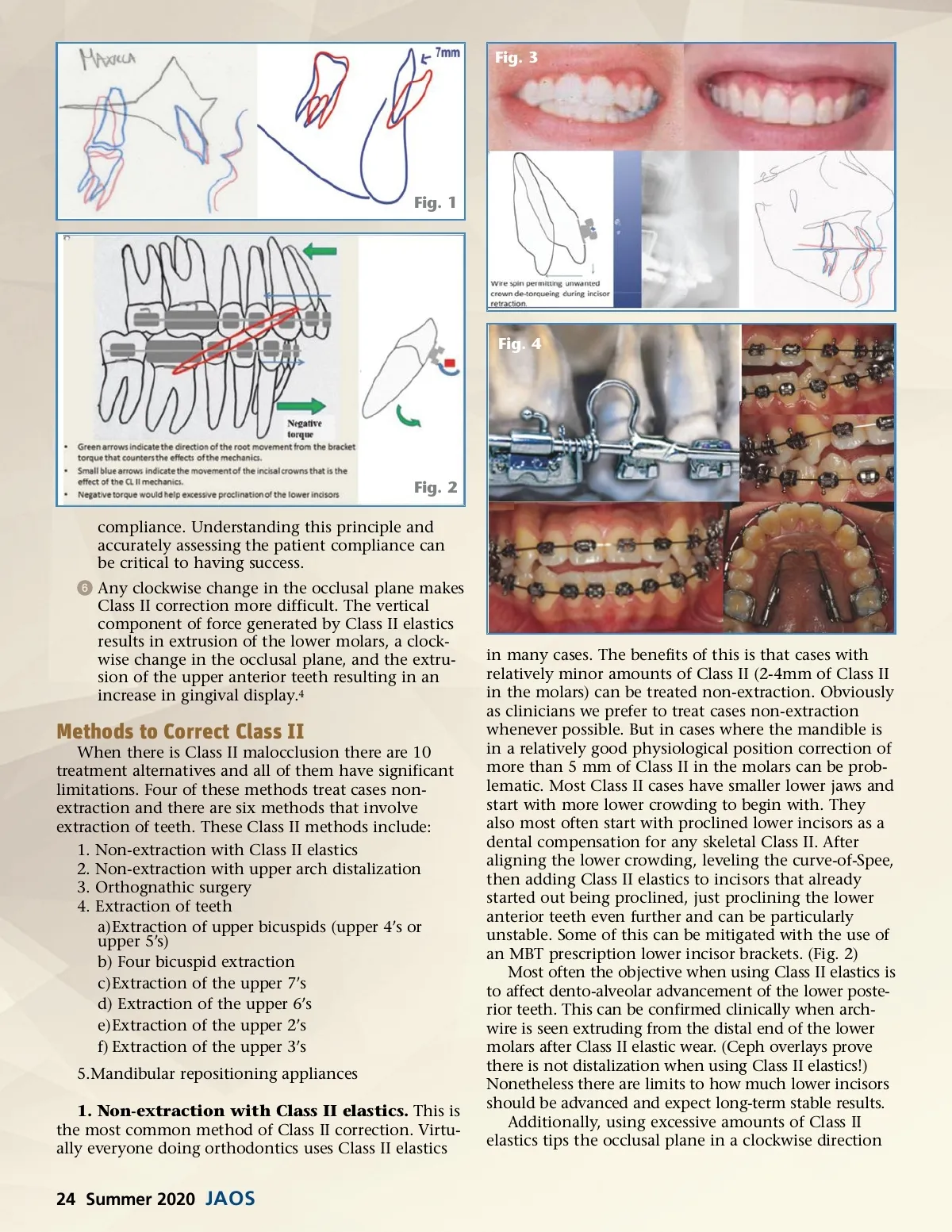
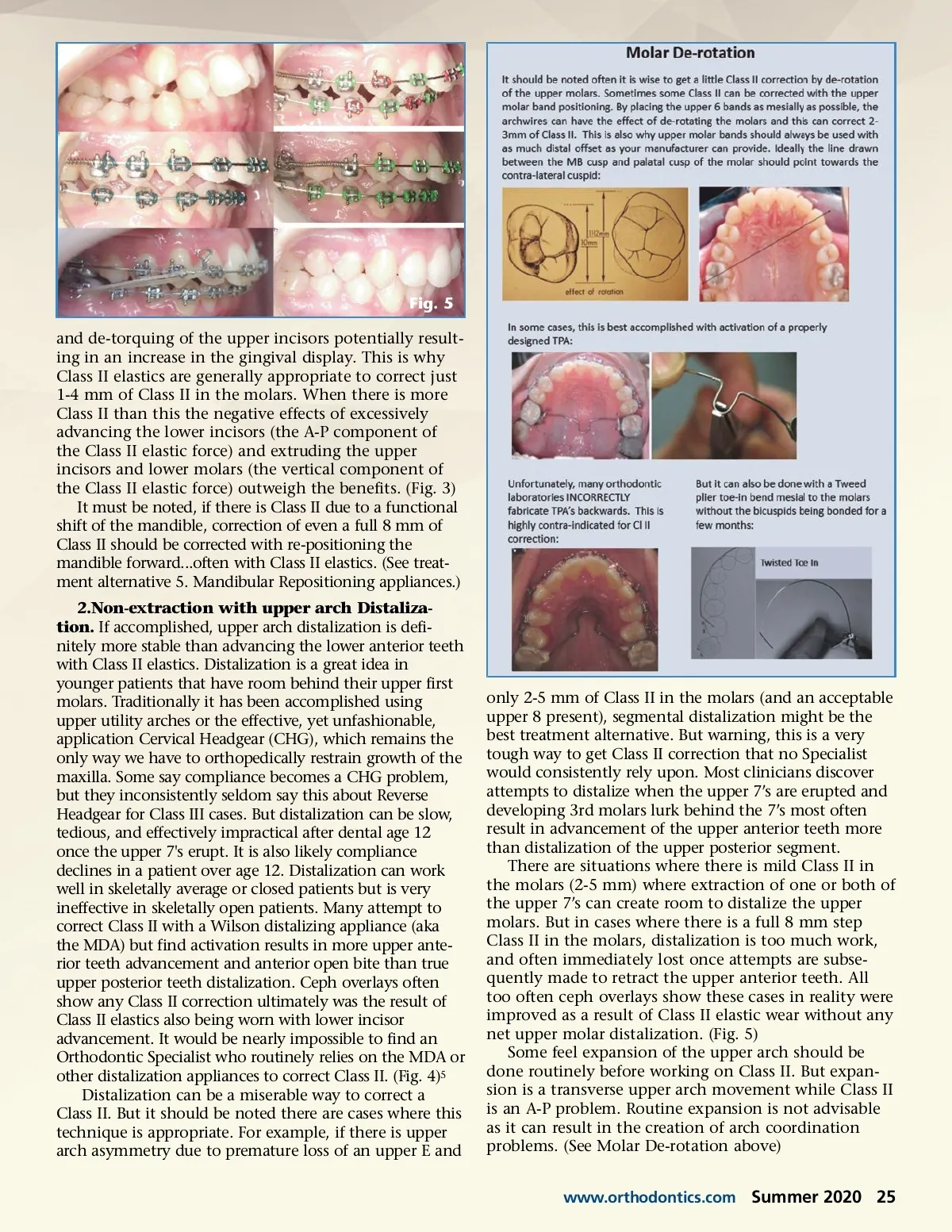
Fig. 5 and de-torquing of the upper incisors potentially result-ing in an increase in the gingival display. This is why Class II elastics are generally appropriate to correct just 1-4 mm of Class II in the molars. When there is more Class II than this the negative effects of excessively advancing the lower incisors (the A-P component of the Class II elastic force) and extruding the upper incisors and lower molars (the vertical component of the Class II elastic force) outweigh the benefits. (Fig. 3) It must be noted, if there is Class II due to a functional shift of the mandible, correction of even a full 8 mm of Class II should be corrected with re-positioning the mandible forward...often with Class II elastics. (See treat-ment alternative 5. Mandibular Repositioning appliances.) 2.Non-extraction with upper arch Distaliza-tion. If accomplished, upper arch distalization is defi-nitely more stable than advancing the lower anterior teeth with Class II elastics. Distalization is a great idea in younger patients that have room behind their upper first molars. Traditionally it has been accomplished using upper utility arches or the effective, yet unfashionable, application Cervical Headgear (CHG), which remains the only way we have to orthopedically restrain growth of the maxilla. Some say compliance becomes a CHG problem, but they inconsistently seldom say this about Reverse Headgear for Class III cases. But distalization can be slow, tedious, and effectively impractical after dental age 12 once the upper 7's erupt. It is also likely compliance declines in a patient over age 12. Distalization can work well in skeletally average or closed patients but is very ineffective in skeletally open patients. Many attempt to correct Class II with a Wilson distalizing appliance (aka the MDA) but find activation results in more upper ante-rior teeth advancement and anterior open bite than true upper posterior teeth distalization. Ceph overlays often show any Class II correction ultimately was the result of Class II elastics also being worn with lower incisor advancement. It would be nearly impossible to find an Orthodontic Specialist who routinely relies on the MDA or other distalization appliances to correct Class II. (Fig. 4) 5 Distalization can be a miserable way to correct a Class II. But it should be noted there are cases where this technique is appropriate. For example, if there is upper arch asymmetry due to premature loss of an upper E and only 2-5 mm of Class II in the molars (and an acceptable upper 8 present), segmental distalization might be the best treatment alternative. But warning, this is a very tough way to get Class II correction that no Specialist would consistently rely upon. Most clinicians discover attempts to distalize when the upper 7’s are erupted and developing 3rd molars lurk behind the 7’s most often result in advancement of the upper anterior teeth more than distalization of the upper posterior segment. There are situations where there is mild Class II in the molars (2-5 mm) where extraction of one or both of the upper 7’s can create room to distalize the upper molars. But in cases where there is a full 8 mm step Class II in the molars, distalization is too much work, and often immediately lost once attempts are subse-quently made to retract the upper anterior teeth. All too often ceph overlays show these cases in reality were improved as a result of Class II elastic wear without any net upper molar distalization. (Fig. 5) Some feel expansion of the upper arch should be done routinely before working on Class II. But expan-sion is a transverse upper arch movement while Class II is an A-P problem. Routine expansion is not advisable as it can result in the creation of arch coordination problems. (See Molar De-rotation above) www.orthodontics.com Summer 2020 25
Journal of the American Orthodontic Society Summer 2020: Page 25