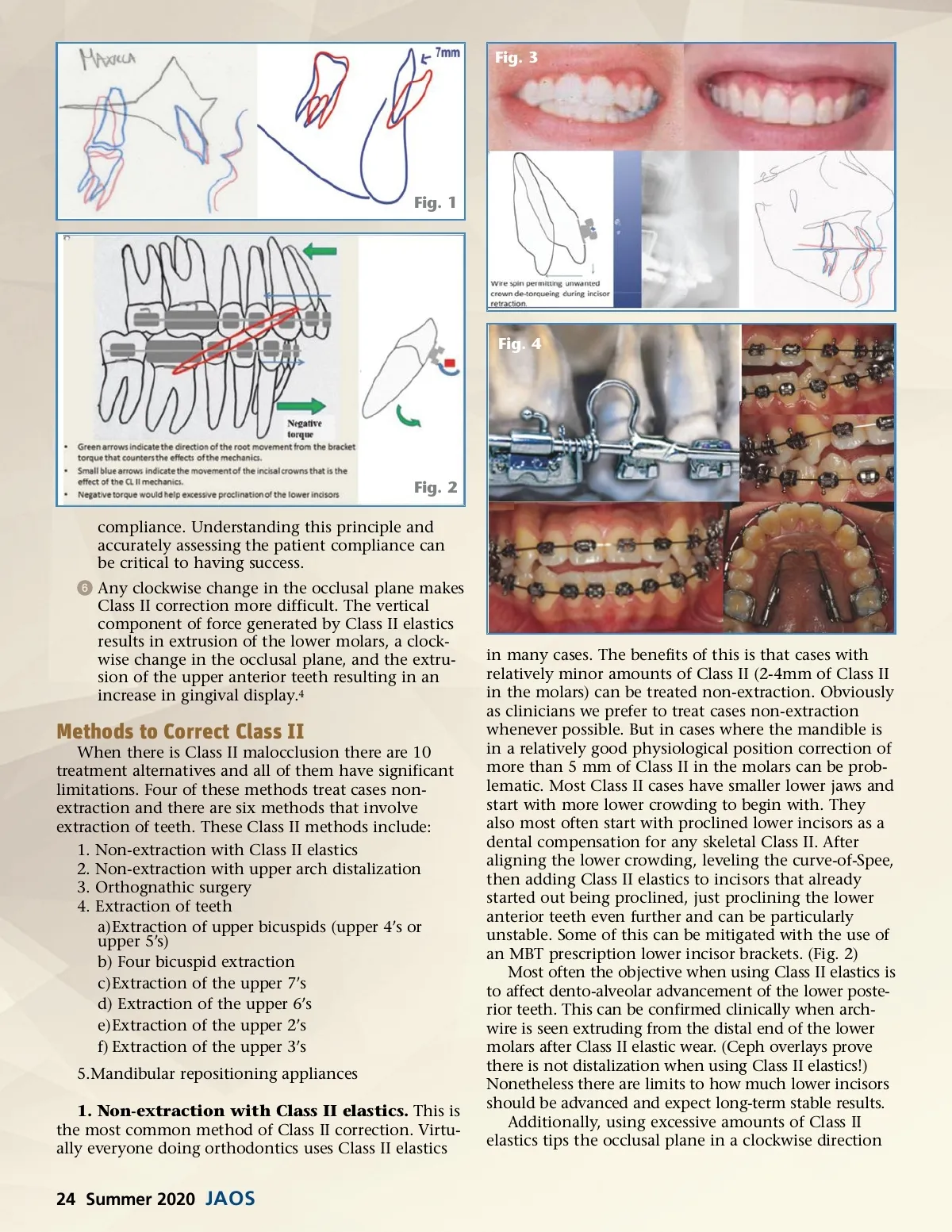
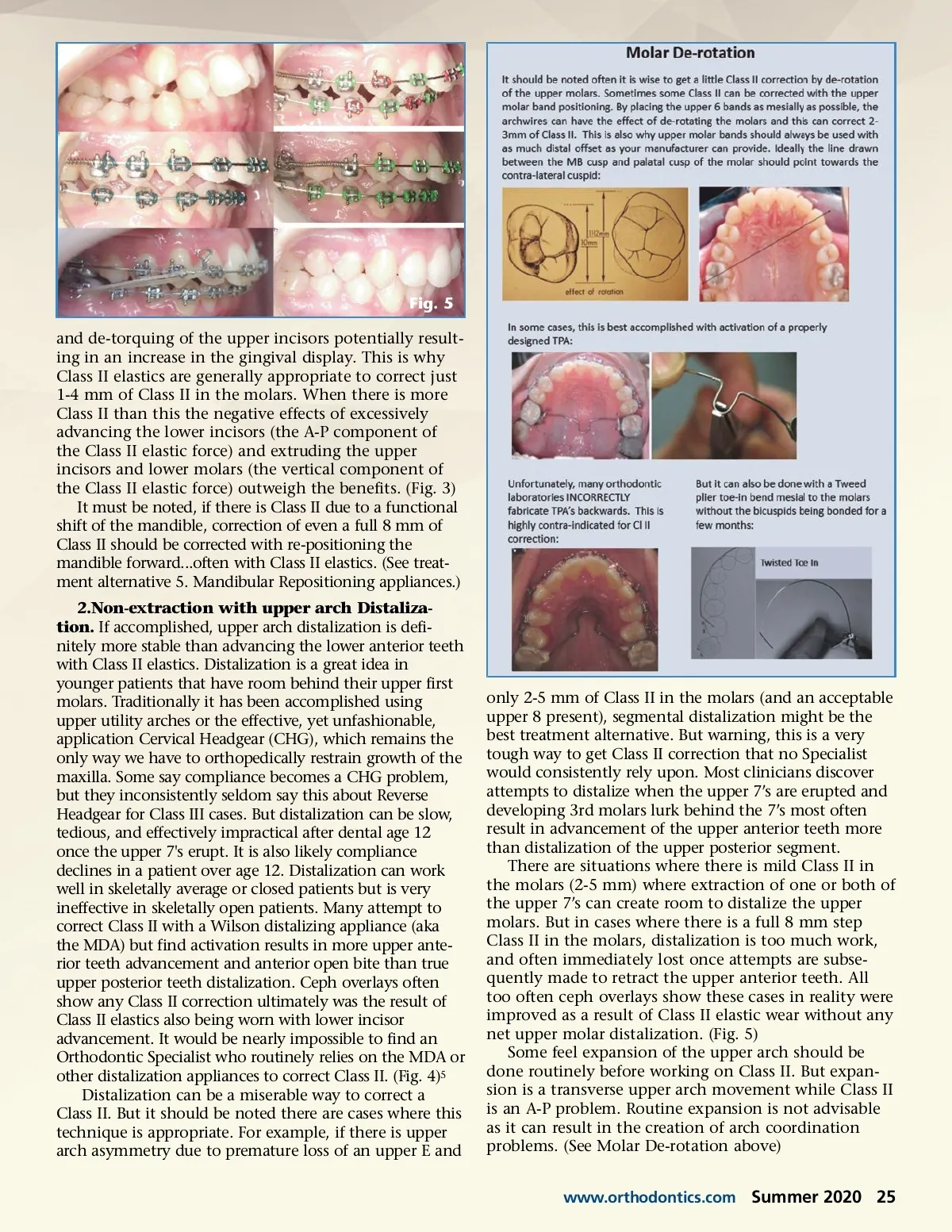
Fig. 3 Fig. 1 Fig. 4 Fig. 2 compliance. Understanding this principle and accurately assessing the patient compliance can be critical to having success. ᕦ Any clockwise change in the occlusal plane makes Class II correction more difficult. The vertical component of force generated by Class II elastics results in extrusion of the lower molars, a clock-wise change in the occlusal plane, and the extru-sion of the upper anterior teeth resulting in an increase in gingival display. 4 Methods to Correct Class II When there is Class II malocclusion there are 10 treatment alternatives and all of them have significant limitations. Four of these methods treat cases non-extraction and there are six methods that involve extraction of teeth. These Class II methods include: 1. Non-extraction with Class II elastics 2. Non-extraction with upper arch distalization 3. Orthognathic surgery 4. Extraction of teeth a)Extraction of upper bicuspids (upper 4’s or upper 5’s) b) Four bicuspid extraction c)Extraction of the upper 7’s d) Extraction of the upper 6’s e)Extraction of the upper 2’s f) Extraction of the upper 3’s 5.Mandibular repositioning appliances 1. Non-extraction with Class II elastics. This is the most common method of Class II correction. Virtu-ally everyone doing orthodontics uses Class II elastics in many cases. The benefits of this is that cases with relatively minor amounts of Class II (2-4mm of Class II in the molars) can be treated non-extraction. Obviously as clinicians we prefer to treat cases non-extraction whenever possible. But in cases where the mandible is in a relatively good physiological position correction of more than 5 mm of Class II in the molars can be prob-lematic. Most Class II cases have smaller lower jaws and start with more lower crowding to begin with. They also most often start with proclined lower incisors as a dental compensation for any skeletal Class II. After aligning the lower crowding, leveling the curve-of-Spee, then adding Class II elastics to incisors that already started out being proclined, just proclining the lower anterior teeth even further and can be particularly unstable. Some of this can be mitigated with the use of an MBT prescription lower incisor brackets. (Fig. 2) Most often the objective when using Class II elastics is to affect dento-alveolar advancement of the lower poste-rior teeth. This can be confirmed clinically when arch-wire is seen extruding from the distal end of the lower molars after Class II elastic wear. (Ceph overlays prove there is not distalization when using Class II elastics!) Nonetheless there are limits to how much lower incisors should be advanced and expect long-term stable results. Additionally, using excessive amounts of Class II elastics tips the occlusal plane in a clockwise direction 24 Summer 2020 JAOS
Journal of the American Orthodontic Society Summer 2020: Page 24