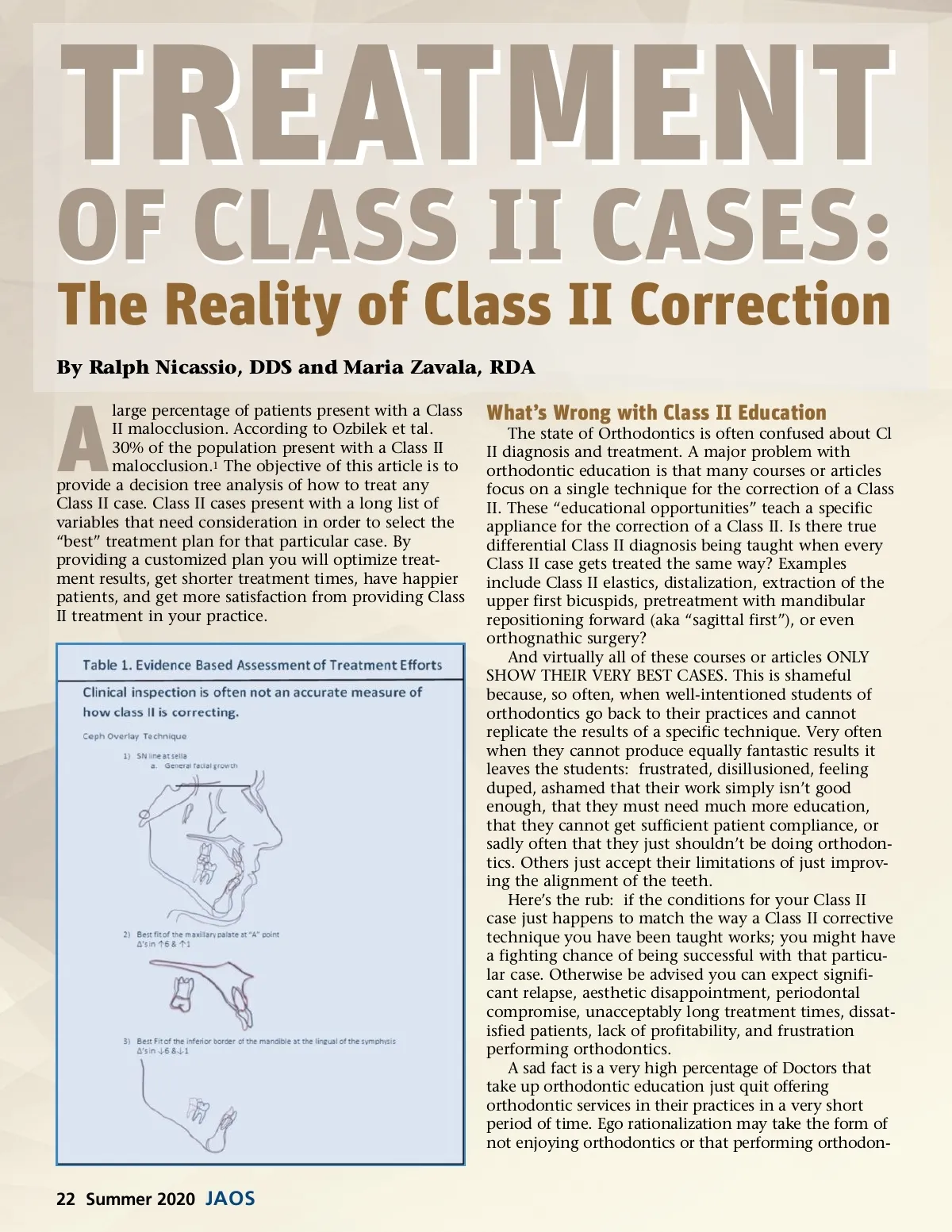
tics “just isn’t profitable.” (Has anyone ever seen a skilled Orthodontic Specialist that wasn’t highly profitable?) To translate what this means is to understand these well-intentioned General Practitioners simply could not get good enough results to feel good about the orthodontic work they were producing, that they simply could not finish cases in a timely fashion, or that they were simply losing sleep from the unstable and unsatisfying results of their cases. The problem is exacerbated when they feel there is no real support when results do not match what was promised, if they inevitably run into obstacles, or even trouble. The Challenge of Class II Correction Despite orthodontic mythology, Class II cases are more difficult to treat than Class III cases. Class II cases are difficult to treat for several reasons: ᕡ It is difficult to bring lower posterior teeth forward. The most difficult teeth to move in the lower arch are lower molars. Even more difficult, is bringing the lower 6’s and 5’s forward if the lower 4’s are extracted. And the most challenging feat is affecting dento-alveolar advancement of an entire non-extraction lower arch. Please remember if Class II elastics are administered and wire is observed extruding from the distal end of the lower molars there has been dento-alveolar advancement of the lower posterior teeth. But, on the other hand, if Class II elastics are used and Class II correction ensues without wire extruding from the distal end of the lower molars, the mandible itself bodily came forward. Even if it is appropriate to band/bond the lower 7’s early in a case, perhaps to facilitate alignment or arch coordination, it is truly counter-produc-tive to extend lower archwires to the lower 7’s during Class II elastics mechanics to effect dento-alveolar advancement of the lower dentition. The added additional friction of extending a lower archwire to the lower 7’s creates excessive lower posterior anchorage. ᕢ Upper posterior teeth can come forward too easily. This is why great care should be made to avoid any upper intra-arch mechanics to close spaces or to reduce overjet. The hidden anchorage of the cortical plate of the palate can result in the upper posterior teeth coming forward with the use of power chain or upper intra-arch closing coils. This is why in Class II cases that are treated with upper extractions, banding/bonding the upper 6’s and 7’s and possibly adding a Transpalatal Arch (TPA) to maximize the upper posterior anchorage is wise. ᕣ Not all mandibles need to be postured forward. Many patients have condyles in a perfectly normal physiological position. This is why attempts to posture mandible forward in many Class II cases results in Class II relapse. Techniques that require lifetime retention using an anterior bite block to posture the mandible forward have not produced stable Class II correction. ᕤ Understanding appliance design including bracket torque prescription is essential. Cases needing the upper anterior teeth retracted are often best treated with upper incisor brackets with a High torque and not a Roth nor an MBT prescription. Failure to understand this can easily incorrectly conclude that upper extractions can lead to ruin-ing a profile of a face. ᕥ Anything done between the arches (inter-arch forces) requires some level of patient compliance. But mechanics done within the same arch (Intra-arch forces) can be achieved without patient www.orthodontics.com Those That Just Ignore Class II The condition of the orthodontic specialty is getting even worse with the nonsensical claim that removable aligners can be a suitable substitute to the fixed appli-ance. And here we include just impeccable alignment of the teeth notwithstanding Class II correction. Has anyone ever seen an aligner case that elicited a “wow” from a trained professional? It’s an unfortunate dumbing down of expectations of results or time required to produce elegant orthodontic results. Still others have no aspiration whatsoever to correct Class II (or Class III) and have rele-gated their orthodontic services to Six Month Smiles, Fast Braces, or a removable aligner treatment protocol. Acknowledgement should be made that many patients do not want braces. But all patients want good results produced in a timely fashion. Some actually expect excellent results and will complain when Class II expresses into overjet after alignment is improved. Let’s also compare results side-by-side of what aligners can do compared to those of a skilled knowledgeable clinical with the fixed appliance. This is especially true when A-P correction is indicated. This article is for those that want to elevate their standard of care to the highest levels. Never mind that many Orthodontists have sold-out their Specialty to the lowest common denominator or that some General Practitioner’s doing orthodontics only aspire to improv-ing the upper “Social Six.”. Evidence-Based Ortho Whatever technique you select to correct Class II (or think you are using!), before/after cephalometric trac-ing must be overlaid to confirm the mechanism of how the Class II was actually corrected. Some claim to be distalizing the upper teeth, when in fact, overlays show they had dento-alveolar advancement of the lower anterior teeth or of repositioning a mandibular forward. Intellectual honesty is the key first step to critically thinking and understanding how A-P correction actu-ally occurred in an orthodontic case. (Table 1) The technique used to correct Class II can make a big difference in the aesthetics, occlusal plane, and stability of a case. The overlays in Figure 1 are examples where Class II correction was truly achieved by distal-ization of the upper posterior teeth compared to where Class II correction was achieved by advancing the lower anterior teeth with Class II elastics. 2,3 Summer 2020 23
Journal of the American Orthodontic Society Summer 2020: Page 23