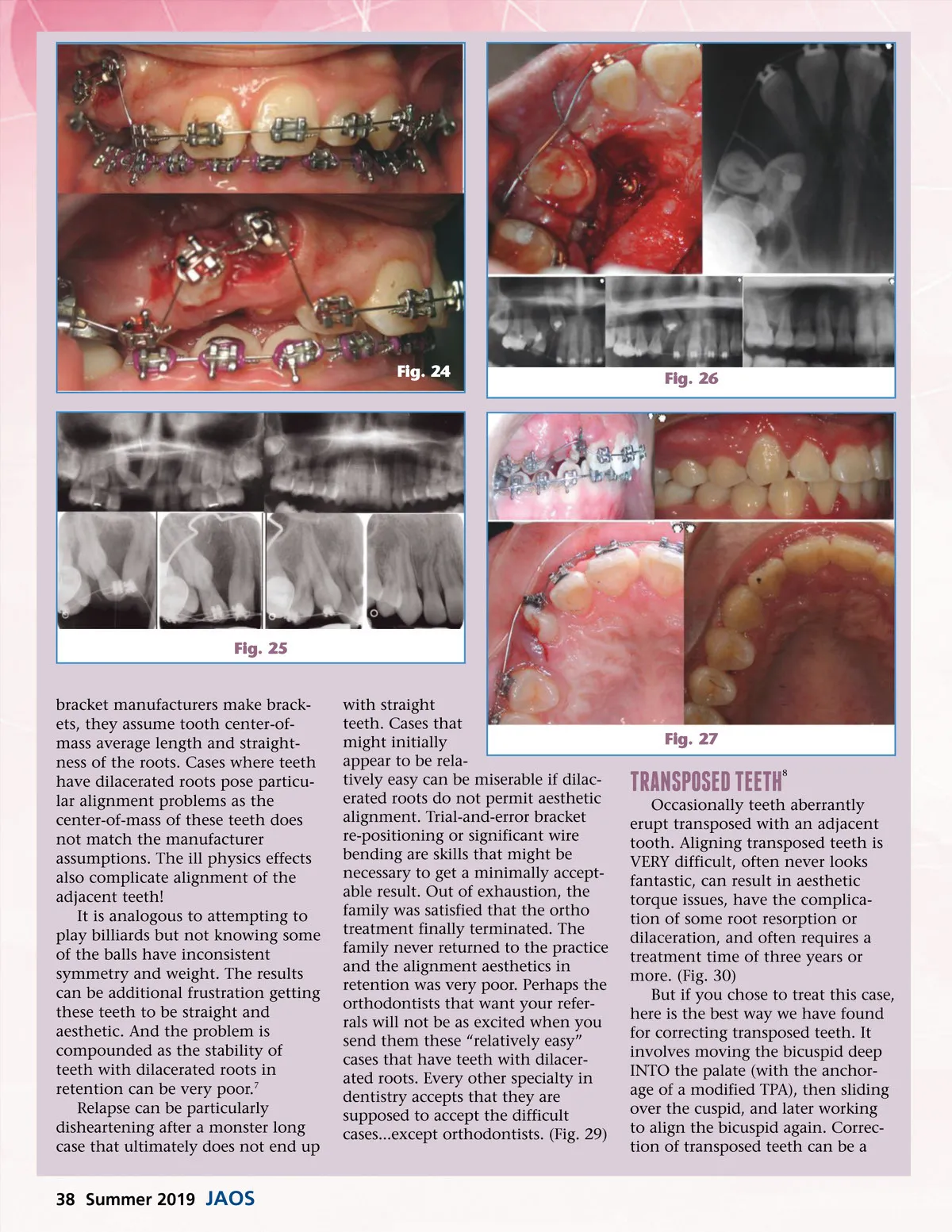
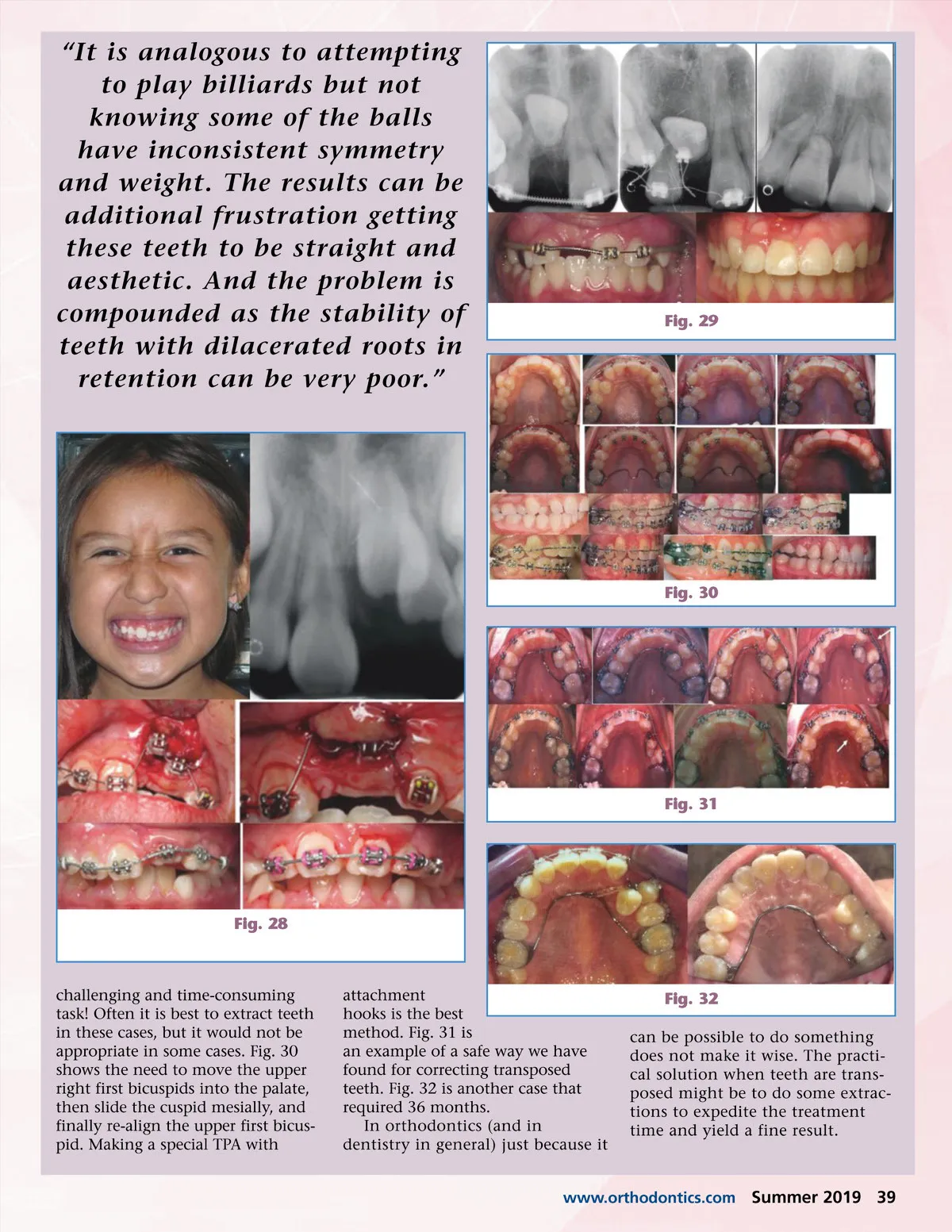
Fig. 24 Fig. 26 Fig. 25 bracket manufacturers make brack-ets, they assume tooth center-of-mass average length and straight-ness of the roots. Cases where teeth have dilacerated roots pose particu-lar alignment problems as the center-of-mass of these teeth does not match the manufacturer assumptions. The ill physics effects also complicate alignment of the adjacent teeth! It is analogous to attempting to play billiards but not knowing some of the balls have inconsistent symmetry and weight. The results can be additional frustration getting these teeth to be straight and aesthetic. And the problem is compounded as the stability of teeth with dilacerated roots in retention can be very poor. 7 Relapse can be particularly disheartening after a monster long case that ultimately does not end up with straight teeth. Cases that might initially appear to be rela-tively easy can be miserable if dilac-erated roots do not permit aesthetic alignment. Trial-and-error bracket re-positioning or significant wire bending are skills that might be necessary to get a minimally accept-able result. Out of exhaustion, the family was satisfied that the ortho treatment finally terminated. The family never returned to the practice and the alignment aesthetics in retention was very poor. Perhaps the orthodontists that want your refer-rals will not be as excited when you send them these “relatively easy” cases that have teeth with dilacer-ated roots. Every other specialty in dentistry accepts that they are supposed to accept the difficult cases...except orthodontists. (Fig. 29) Fig. 27 transposed teeth 8 Occasionally teeth aberrantly erupt transposed with an adjacent tooth. Aligning transposed teeth is VERY difficult, often never looks fantastic, can result in aesthetic torque issues, have the complica-tion of some root resorption or dilaceration, and often requires a treatment time of three years or more. (Fig. 30) But if you chose to treat this case, here is the best way we have found for correcting transposed teeth. It involves moving the bicuspid deep INTO the palate (with the anchor-age of a modified TPA), then sliding over the cuspid, and later working to align the bicuspid again. Correc-tion of transposed teeth can be a 38 Summer 2019 JAOS
Journal of the American Orthodontic Society Summer 2019: Page 38