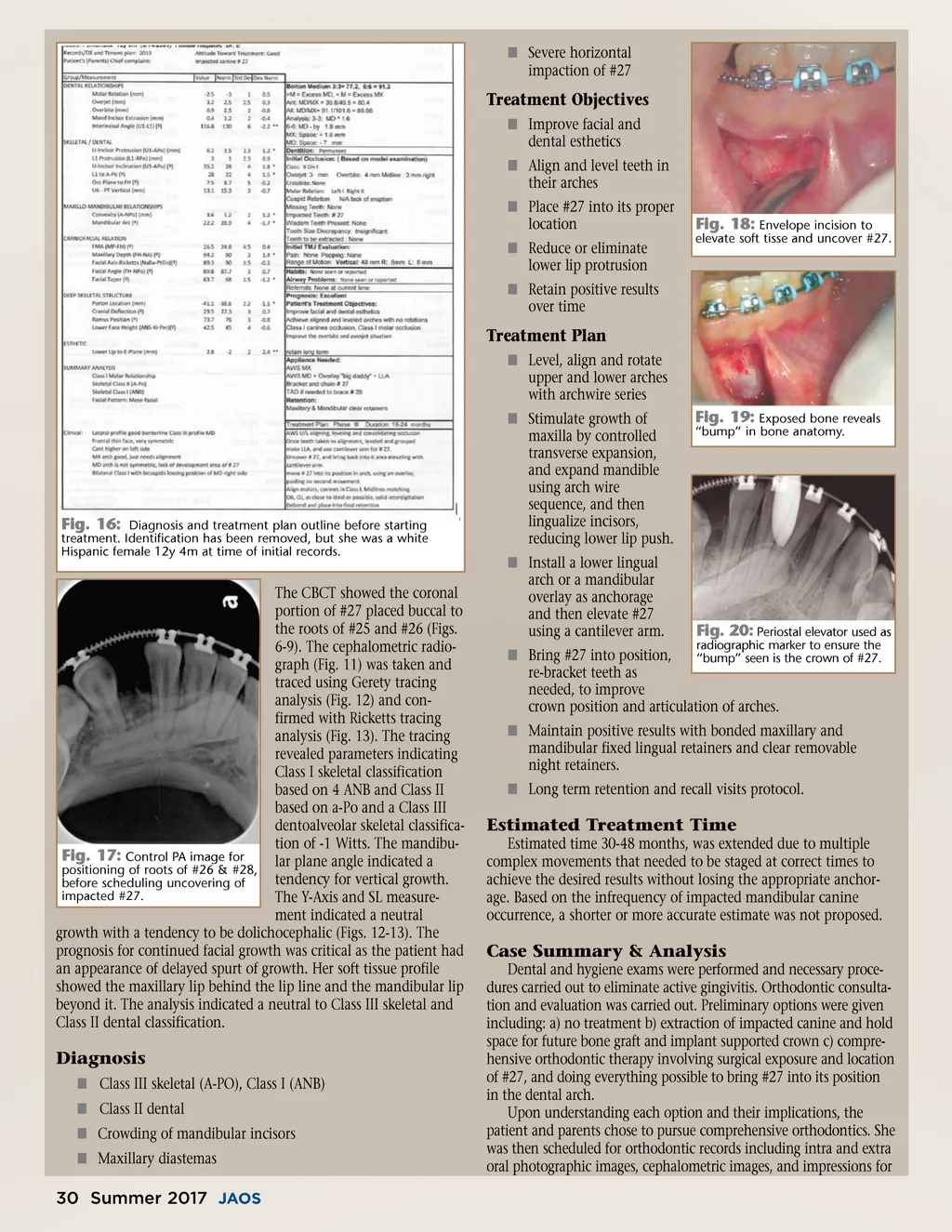
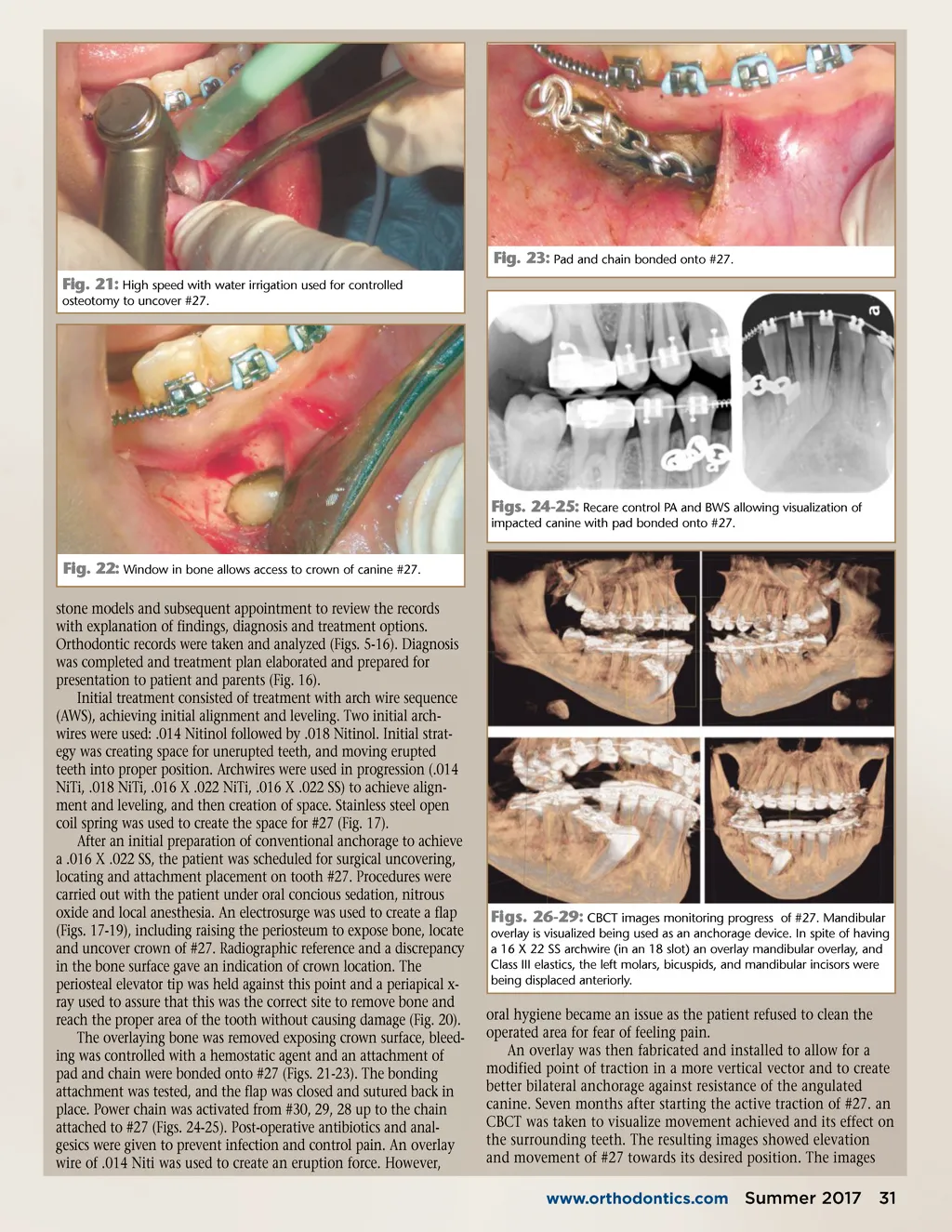
Fig. 23: Pad and chain bonded onto #27. Fig. 21: High speed with water irrigation used for controlled osteotomy to uncover #27. Figs. 24-25: Recare control PA and BWS allowing visualization of impacted canine with pad bonded onto #27. Fig. 22: Window in bone allows access to crown of canine #27. stone models and subsequent appointment to review the records with explanation of findings, diagnosis and treatment options. Orthodontic records were taken and analyzed (Figs. 5-16). Diagnosis was completed and treatment plan elaborated and prepared for presentation to patient and parents (Fig. 16). Initial treatment consisted of treatment with arch wire sequence (AWS), achieving initial alignment and leveling. Two initial arch-wires were used: .014 Nitinol followed by .018 Nitinol. Initial strat-egy was creating space for unerupted teeth, and moving erupted teeth into proper position. Archwires were used in progression (.014 NiTi, .018 NiTi, .016 X .022 NiTi, .016 X .022 SS) to achieve align-ment and leveling, and then creation of space. Stainless steel open coil spring was used to create the space for #27 (Fig. 17). After an initial preparation of conventional anchorage to achieve a .016 X .022 SS, the patient was scheduled for surgical uncovering, locating and attachment placement on tooth #27. Procedures were carried out with the patient under oral concious sedation, nitrous oxide and local anesthesia. An electrosurge was used to create a flap (Figs. 17-19), including raising the periosteum to expose bone, locate and uncover crown of #27. Radiographic reference and a discrepancy in the bone surface gave an indication of crown location. The periosteal elevator tip was held against this point and a periapical x-ray used to assure that this was the correct site to remove bone and reach the proper area of the tooth without causing damage (Fig. 20). The overlaying bone was removed exposing crown surface, bleed-ing was controlled with a hemostatic agent and an attachment of pad and chain were bonded onto #27 (Figs. 21-23). The bonding attachment was tested, and the flap was closed and sutured back in place. Power chain was activated from #30, 29, 28 up to the chain attached to #27 (Figs. 24-25). Post-operative antibiotics and anal-gesics were given to prevent infection and control pain. An overlay wire of .014 Niti was used to create an eruption force. However, Figs. 26-29: CBCT images monitoring progress of #27. Mandibular overlay is visualized being used as an anchorage device. In spite of having a 16 X 22 SS archwire (in an 18 slot) an overlay mandibular overlay, and Class III elastics, the left molars, bicuspids, and mandibular incisors were being displaced anteriorly. oral hygiene became an issue as the patient refused to clean the operated area for fear of feeling pain. An overlay was then fabricated and installed to allow for a modified point of traction in a more vertical vector and to create better bilateral anchorage against resistance of the angulated canine. Seven months after starting the active traction of #27. an CBCT was taken to visualize movement achieved and its effect on the surrounding teeth. The resulting images showed elevation and movement of #27 towards its desired position. The images www.orthodontics.com Summer 2017 31
Journal of the American Orthodontic Society Summer 2017/Buyer's Guide: Page 31