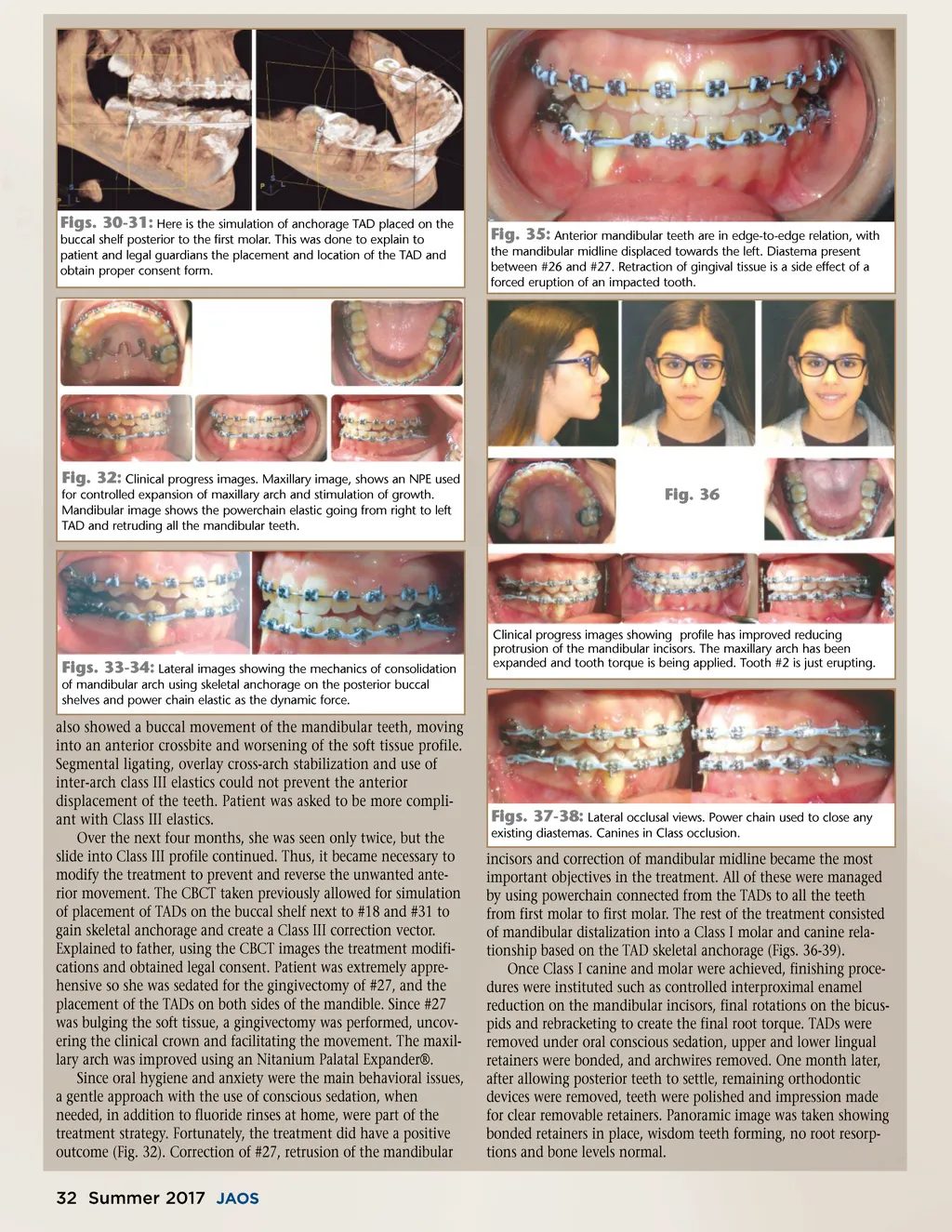
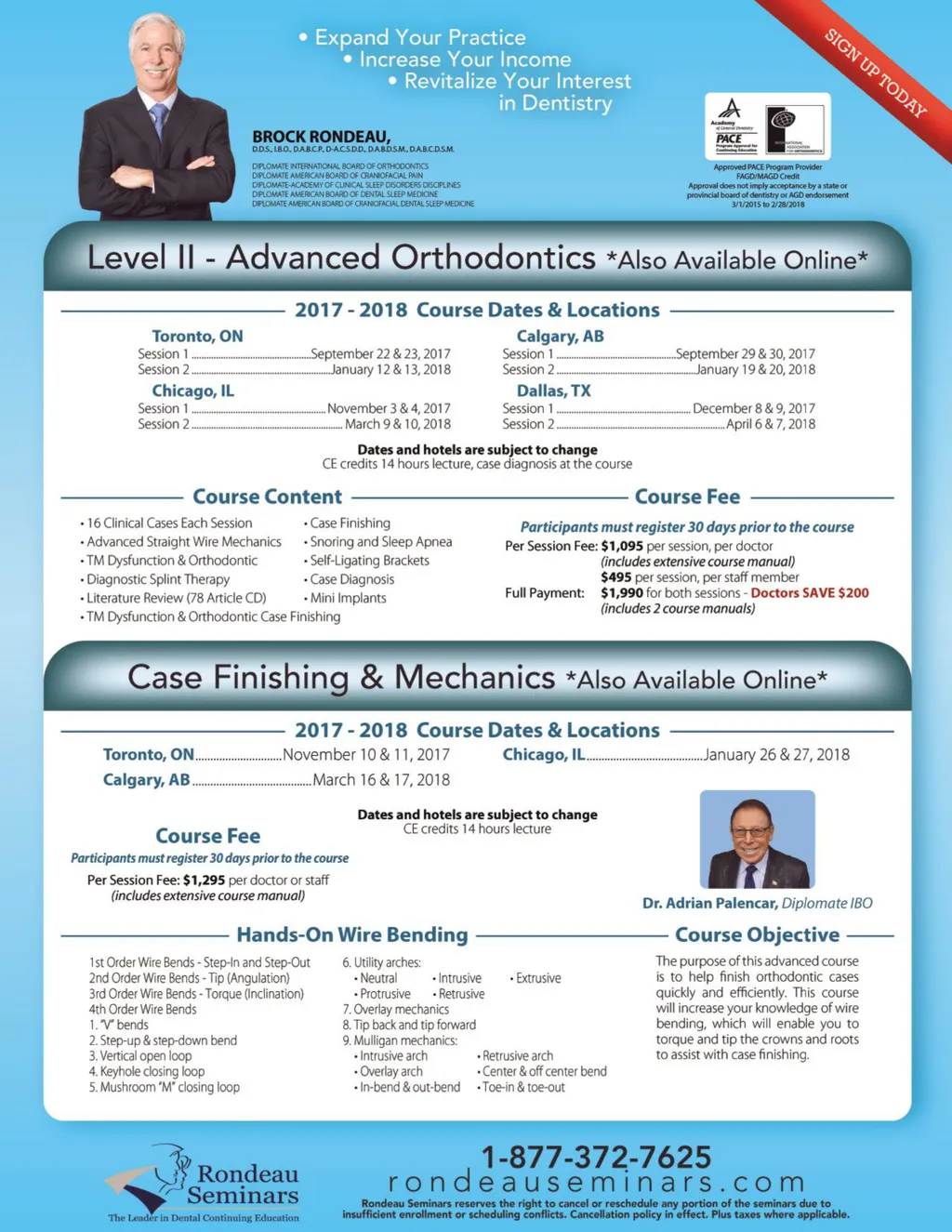
Figs. 30-31: Here is the simulation of anchorage TAD placed on the buccal shelf posterior to the first molar. This was done to explain to patient and legal guardians the placement and location of the TAD and obtain proper consent form. Fig. 35: Anterior mandibular teeth are in edge-to-edge relation, with the mandibular midline displaced towards the left. Diastema present between #26 and #27. Retraction of gingival tissue is a side effect of a forced eruption of an impacted tooth. Fig. 32: Clinical progress images. Maxillary image, shows an NPE used for controlled expansion of maxillary arch and stimulation of growth. Mandibular image shows the powerchain elastic going from right to left TAD and retruding all the mandibular teeth. Fig. 36 Figs. 33-34: Lateral images showing the mechanics of consolidation of mandibular arch using skeletal anchorage on the posterior buccal shelves and power chain elastic as the dynamic force. also showed a buccal movement of the mandibular teeth, moving into an anterior crossbite and worsening of the soft tissue profile. Segmental ligating, overlay cross-arch stabilization and use of inter-arch class III elastics could not prevent the anterior displacement of the teeth. Patient was asked to be more compli-ant with Class III elastics. Over the next four months, she was seen only twice, but the slide into Class III profile continued. Thus, it became necessary to modify the treatment to prevent and reverse the unwanted ante-rior movement. The CBCT taken previously allowed for simulation of placement of TADs on the buccal shelf next to #18 and #31 to gain skeletal anchorage and create a Class III correction vector. Explained to father, using the CBCT images the treatment modifi-cations and obtained legal consent. Patient was extremely appre-hensive so she was sedated for the gingivectomy of #27, and the placement of the TADs on both sides of the mandible. Since #27 was bulging the soft tissue, a gingivectomy was performed, uncov-ering the clinical crown and facilitating the movement. The maxil-lary arch was improved using an Nitanium Palatal Expander®. Since oral hygiene and anxiety were the main behavioral issues, a gentle approach with the use of conscious sedation, when needed, in addition to fluoride rinses at home, were part of the treatment strategy. Fortunately, the treatment did have a positive outcome (Fig. 32). Correction of #27, retrusion of the mandibular Clinical progress images showing profile has improved reducing protrusion of the mandibular incisors. The maxillary arch has been expanded and tooth torque is being applied. Tooth #2 is just erupting. Figs. 37-38: Lateral occlusal views. Power chain used to close any existing diastemas. Canines in Class occlusion. incisors and correction of mandibular midline became the most important objectives in the treatment. All of these were managed by using powerchain connected from the TADs to all the teeth from first molar to first molar. The rest of the treatment consisted of mandibular distalization into a Class I molar and canine rela-tionship based on the TAD skeletal anchorage (Figs. 36-39). Once Class I canine and molar were achieved, finishing proce-dures were instituted such as controlled interproximal enamel reduction on the mandibular incisors, final rotations on the bicus-pids and rebracketing to create the final root torque. TADs were removed under oral conscious sedation, upper and lower lingual retainers were bonded, and archwires removed. One month later, after allowing posterior teeth to settle, remaining orthodontic devices were removed, teeth were polished and impression made for clear removable retainers. Panoramic image was taken showing bonded retainers in place, wisdom teeth forming, no root resorp-tions and bone levels normal. 32 Summer 2017 JAOS
Journal of the American Orthodontic Society Summer 2017/Buyer's Guide: Page 32