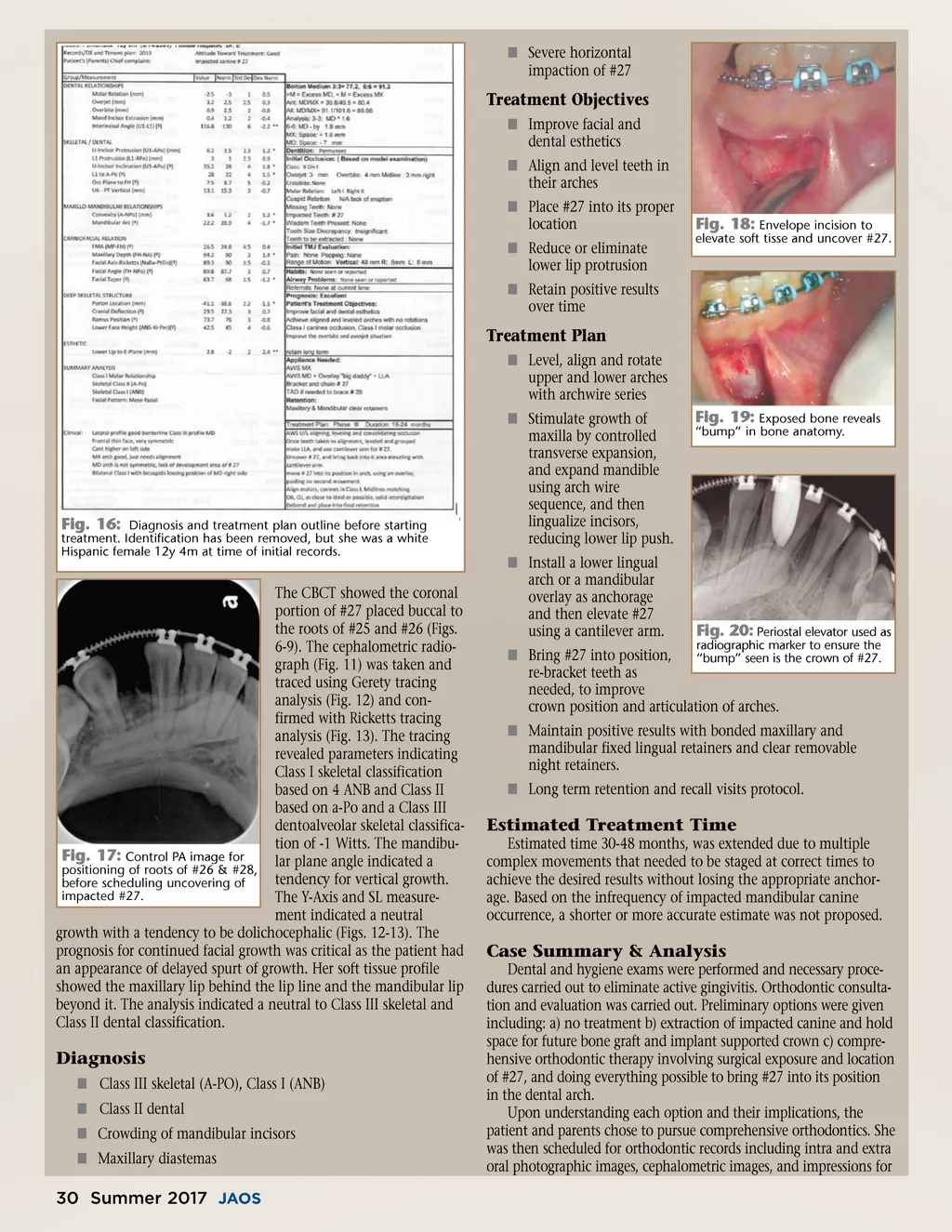
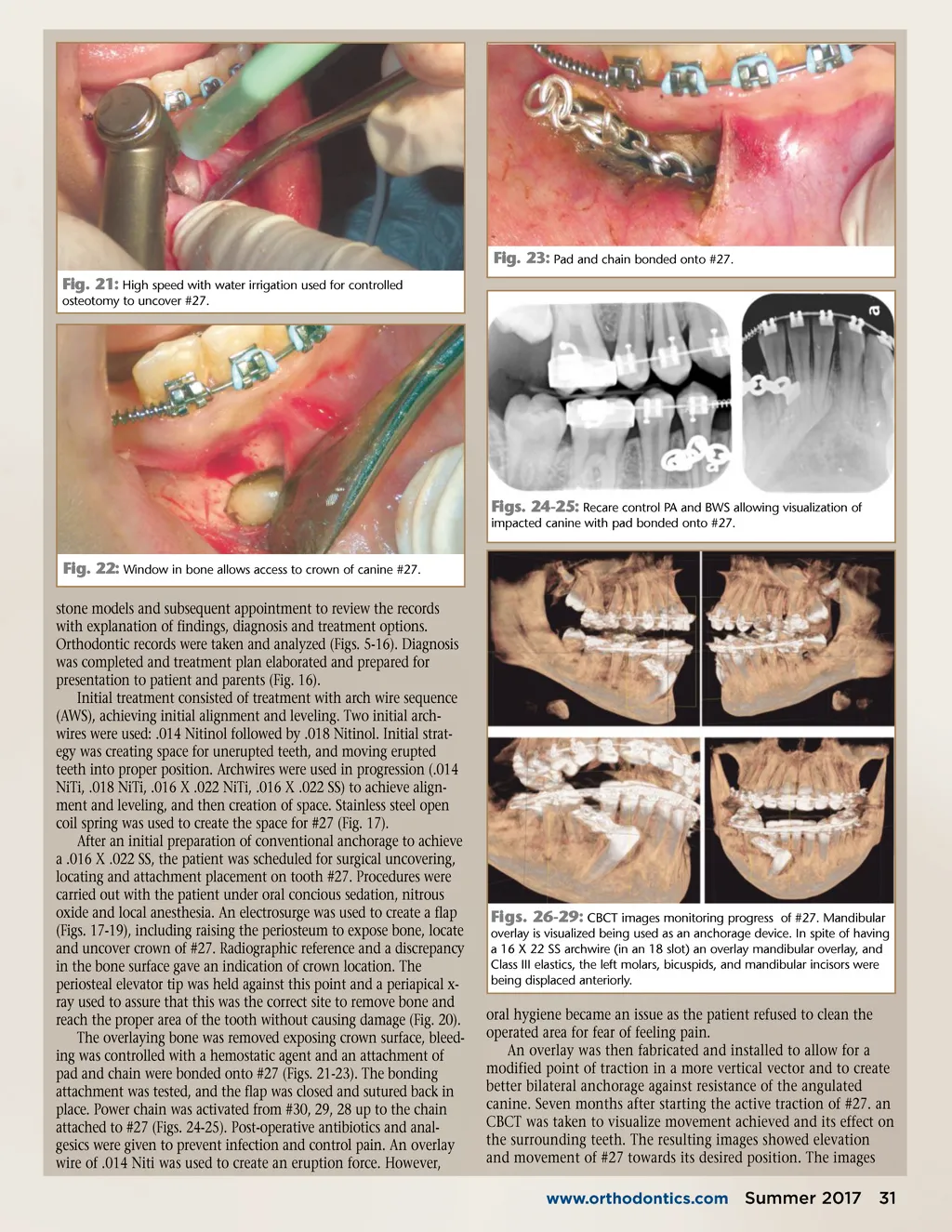
í Severe horizontal impaction of #27 Treatment Objectives í Improve facial and dental esthetics í Align and level teeth in their arches í Place #27 into its proper location í Reduce or eliminate lower lip protrusion í Retain positive results over time Fig. 18: Envelope incision to elevate soft tisse and uncover #27. Treatment Plan í Level, align and rotate upper and lower arches with archwire series í Stimulate growth of maxilla by controlled transverse expansion, and expand mandible using arch wire sequence, and then lingualize incisors, reducing lower lip push. í Install a lower lingual arch or a mandibular overlay as anchorage and then elevate #27 using a cantilever arm. Fig. 19: Exposed bone reveals “bump” in bone anatomy. Fig. 16: Diagnosis and treatment plan outline before starting treatment. Identification has been removed, but she was a white Hispanic female 12y 4m at time of initial records. The CBCT showed the coronal portion of #27 placed buccal to the roots of #25 and #26 (Figs. 6-9). The cephalometric radio-graph (Fig. 11) was taken and traced using Gerety tracing analysis (Fig. 12) and con-firmed with Ricketts tracing analysis (Fig. 13). The tracing revealed parameters indicating Class I skeletal classification based on 4 ANB and Class II based on a-Po and a Class III dentoalveolar skeletal classifica-tion of -1 Witts. The mandibu-Fig. 17: Control PA image for lar plane angle indicated a positioning of roots of #26 & #28, tendency for vertical growth. before scheduling uncovering of impacted #27. The Y-Axis and SL measure-ment indicated a neutral growth with a tendency to be dolichocephalic (Figs. 12-13). The prognosis for continued facial growth was critical as the patient had an appearance of delayed spurt of growth. Her soft tissue profile showed the maxillary lip behind the lip line and the mandibular lip beyond it. The analysis indicated a neutral to Class III skeletal and Class II dental classification. í Bring #27 into position, re-bracket teeth as needed, to improve crown position and articulation of arches. Fig. 20: Periostal elevator used as radiographic marker to ensure the “bump” seen is the crown of #27. í Maintain positive results with bonded maxillary and mandibular fixed lingual retainers and clear removable night retainers. í Long term retention and recall visits protocol. Estimated Treatment Time Estimated time 30-48 months, was extended due to multiple complex movements that needed to be staged at correct times to achieve the desired results without losing the appropriate anchor-age. Based on the infrequency of impacted mandibular canine occurrence, a shorter or more accurate estimate was not proposed. Case Summary & Analysis Dental and hygiene exams were performed and necessary proce-dures carried out to eliminate active gingivitis. Orthodontic consulta-tion and evaluation was carried out. Preliminary options were given including: a) no treatment b) extraction of impacted canine and hold space for future bone graft and implant supported crown c) compre-hensive orthodontic therapy involving surgical exposure and location of #27, and doing everything possible to bring #27 into its position in the dental arch. Upon understanding each option and their implications, the patient and parents chose to pursue comprehensive orthodontics. She was then scheduled for orthodontic records including intra and extra oral photographic images, cephalometric images, and impressions for Diagnosis í Class III skeletal (A-PO), Class I (ANB) í Class II dental í Crowding of mandibular incisors í Maxillary diastemas 30 Summer 2017 JAOS
Journal of the American Orthodontic Society Summer 2017/Buyer's Guide: Page 30