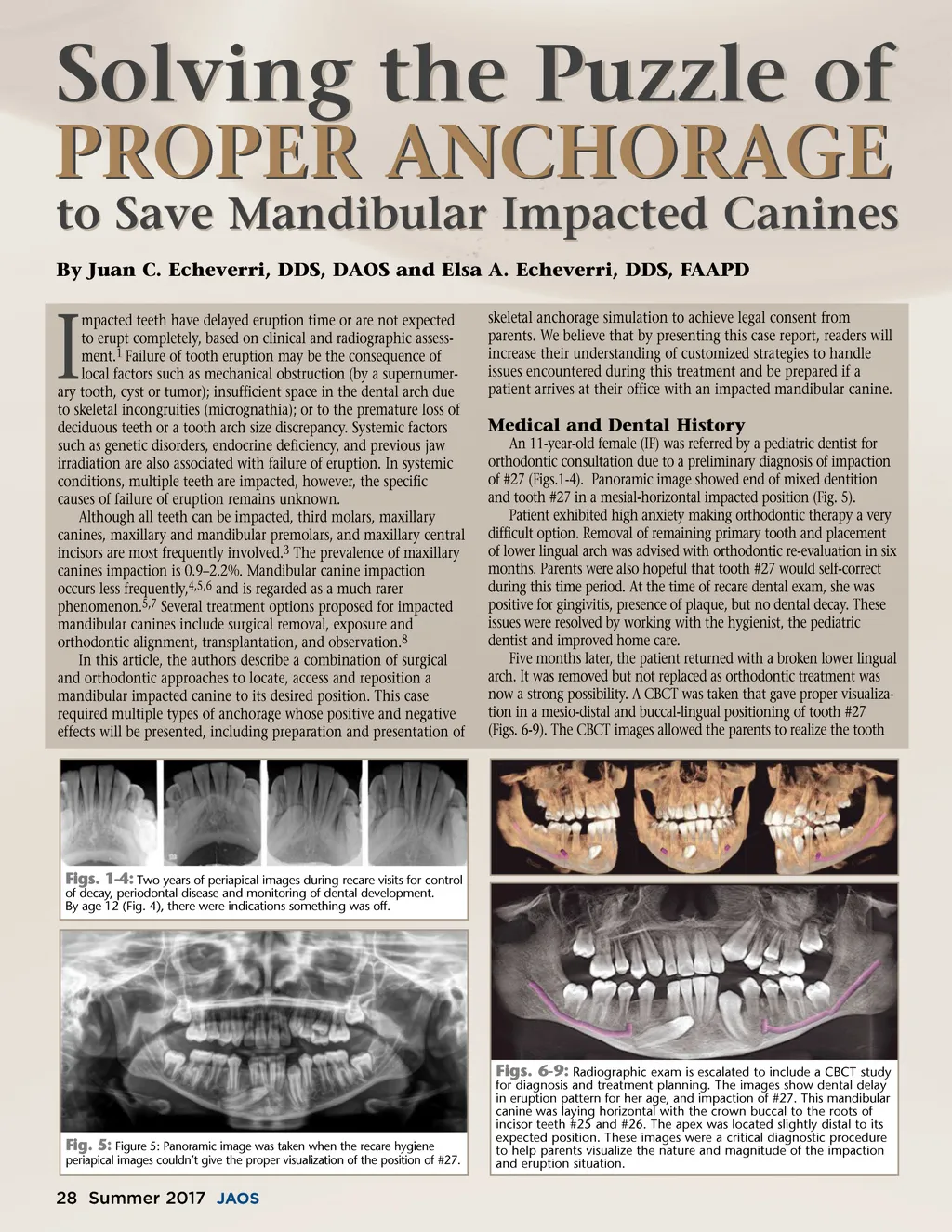
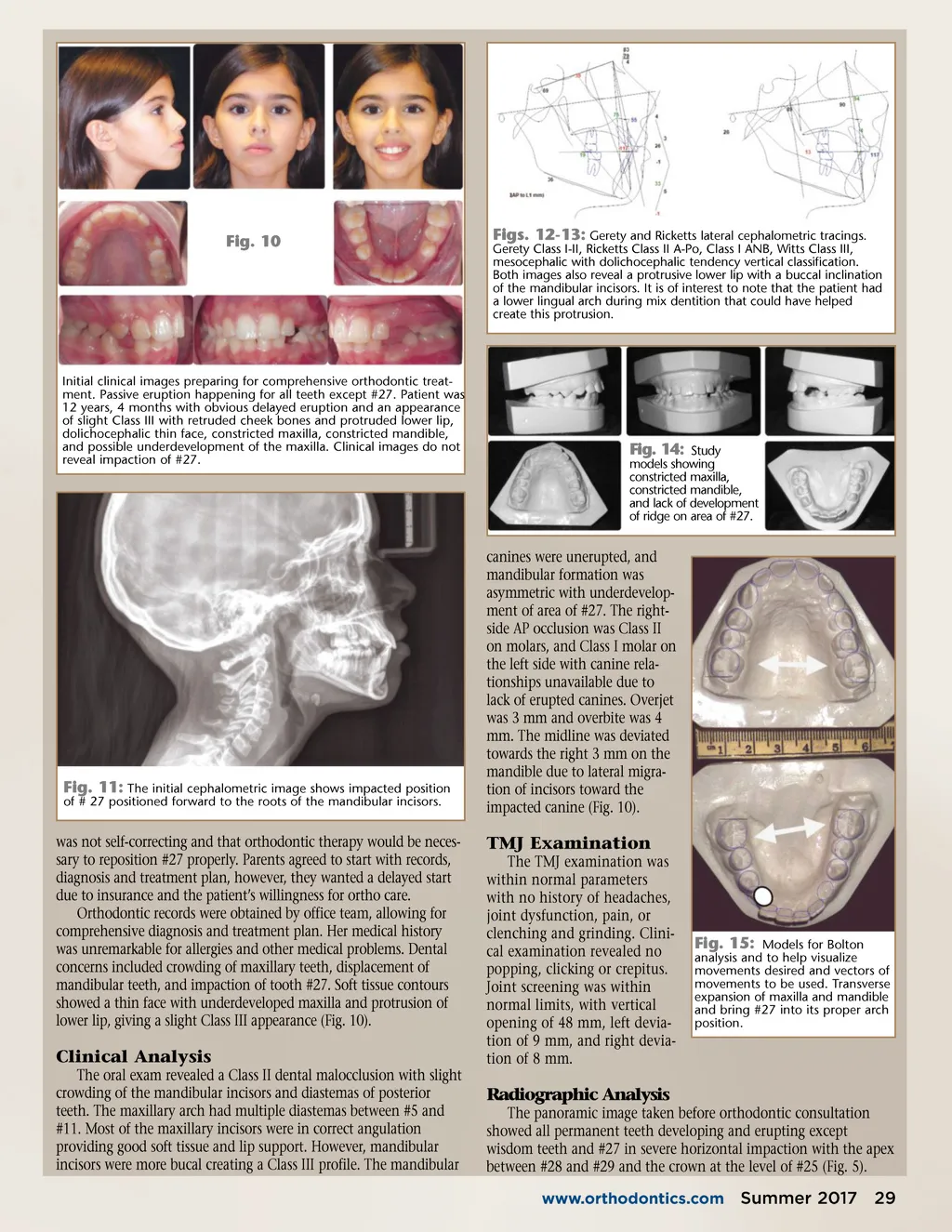
Fig. 10 Figs. 12-13: Gerety and Ricketts lateral cephalometric tracings. Gerety Class I-II, Ricketts Class II A-Po, Class I ANB, Witts Class III, mesocephalic with dolichocephalic tendency vertical classification. Both images also reveal a protrusive lower lip with a buccal inclination of the mandibular incisors. It is of interest to note that the patient had a lower lingual arch during mix dentition that could have helped create this protrusion. Initial clinical images preparing for comprehensive orthodontic treat-ment. Passive eruption happening for all teeth except #27. Patient was 12 years, 4 months with obvious delayed eruption and an appearance of slight Class III with retruded cheek bones and protruded lower lip, dolichocephalic thin face, constricted maxilla, constricted mandible, and possible underdevelopment of the maxilla. Clinical images do not reveal impaction of #27. Fig. 14: Study models showing constricted maxilla, constricted mandible, and lack of development of ridge on area of #27. canines were unerupted, and mandibular formation was asymmetric with underdevelop-ment of area of #27. The right-side AP occlusion was Class II on molars, and Class I molar on the left side with canine rela-tionships unavailable due to lack of erupted canines. Overjet was 3 mm and overbite was 4 mm. The midline was deviated towards the right 3 mm on the mandible due to lateral migra-tion of incisors toward the impacted canine (Fig. 10). Fig. 11: The initial cephalometric image shows impacted position of # 27 positioned forward to the roots of the mandibular incisors. was not self-correcting and that orthodontic therapy would be neces-sary to reposition #27 properly. Parents agreed to start with records, diagnosis and treatment plan, however, they wanted a delayed start due to insurance and the patient’s willingness for ortho care. Orthodontic records were obtained by office team, allowing for comprehensive diagnosis and treatment plan. Her medical history was unremarkable for allergies and other medical problems. Dental concerns included crowding of maxillary teeth, displacement of mandibular teeth, and impaction of tooth #27. Soft tissue contours showed a thin face with underdeveloped maxilla and protrusion of lower lip, giving a slight Class III appearance (Fig. 10). TMJ Examination The TMJ examination was within normal parameters with no history of headaches, joint dysfunction, pain, or clenching and grinding. Clini-cal examination revealed no popping, clicking or crepitus. Joint screening was within normal limits, with vertical opening of 48 mm, left devia-tion of 9 mm, and right devia-tion of 8 mm. Fig. 15: Models for Bolton analysis and to help visualize movements desired and vectors of movements to be used. Transverse expansion of maxilla and mandible and bring #27 into its proper arch position. Clinical Analysis The oral exam revealed a Class II dental malocclusion with slight crowding of the mandibular incisors and diastemas of posterior teeth. The maxillary arch had multiple diastemas between #5 and #11. Most of the maxillary incisors were in correct angulation providing good soft tissue and lip support. However, mandibular incisors were more bucal creating a Class III profile. The mandibular Radiographic Analysis The panoramic image taken before orthodontic consultation showed all permanent teeth developing and erupting except wisdom teeth and #27 in severe horizontal impaction with the apex between #28 and #29 and the crown at the level of #25 (Fig. 5). www.orthodontics.com Summer 2017 29
Journal of the American Orthodontic Society Summer 2017/Buyer's Guide: Page 29