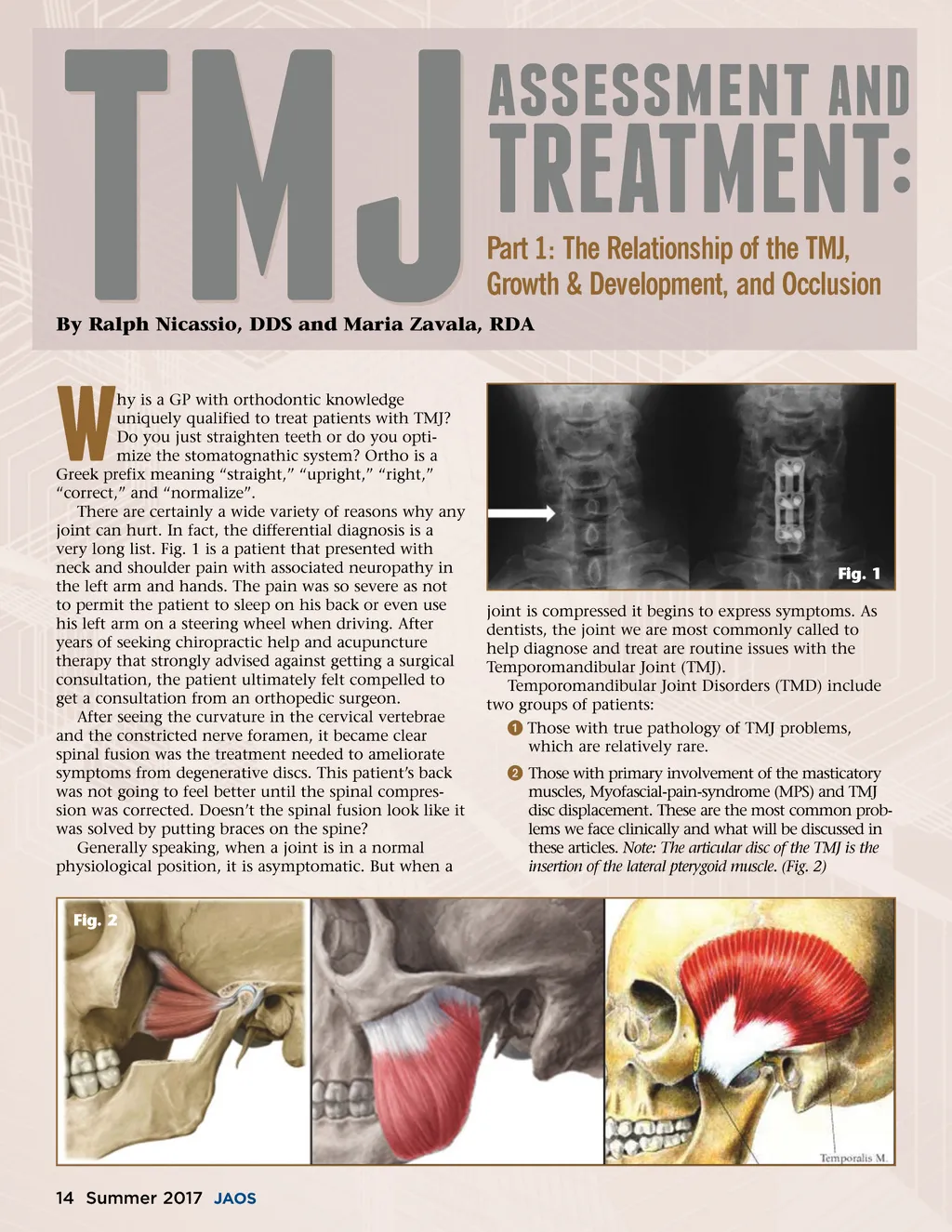
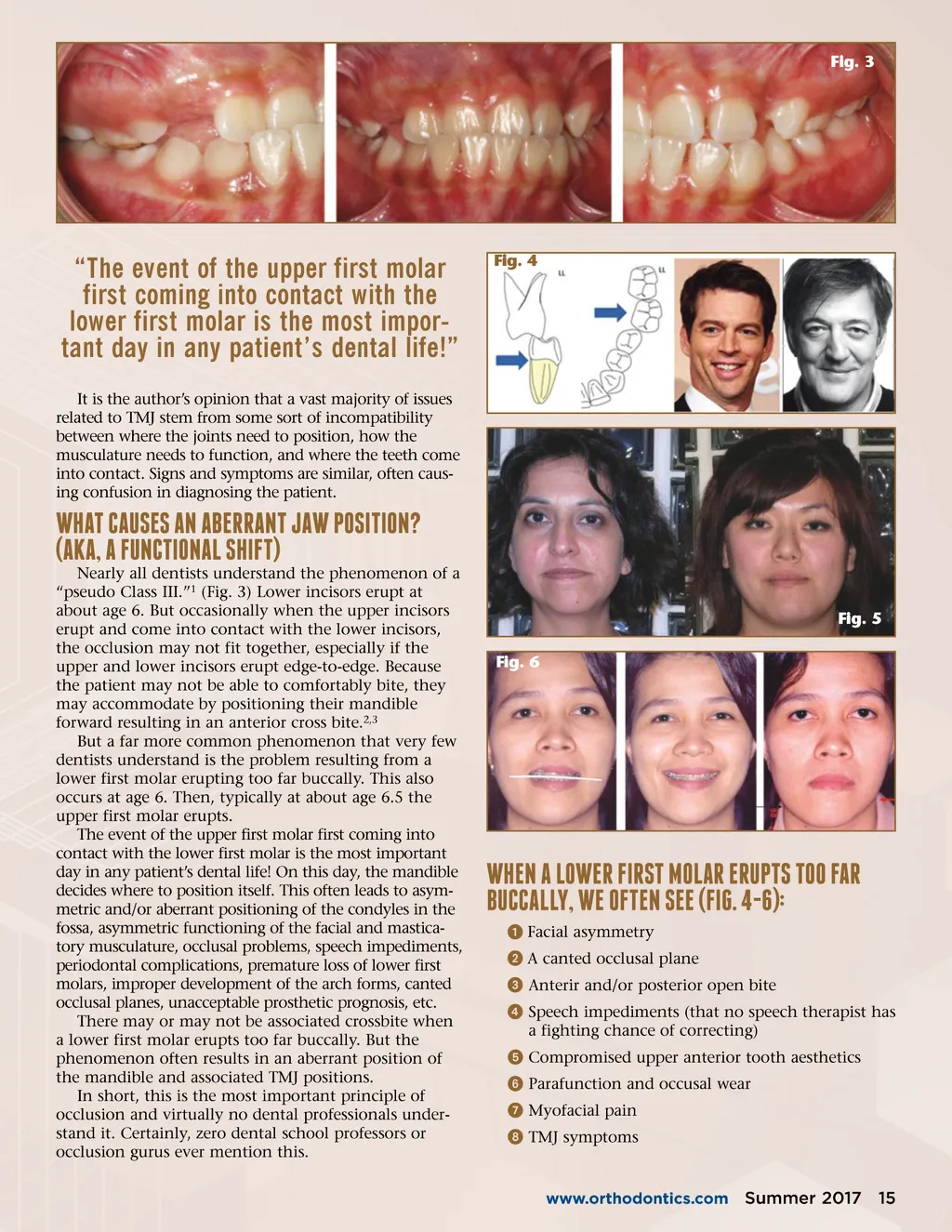
Fig. 3 “The event of the upper first molar first coming into contact with the lower first molar is the most impor-tant day in any patient’s dental life!” It is the author’s opinion that a vast majority of issues related to TMJ stem from some sort of incompatibility between where the joints need to position, how the musculature needs to function, and where the teeth come into contact. Signs and symptoms are similar, often caus-ing confusion in diagnosing the patient. Fig. 4 Nearly all dentists understand the phenomenon of a “pseudo Class III.” 1 (Fig. 3) Lower incisors erupt at about age 6. But occasionally when the upper incisors erupt and come into contact with the lower incisors, the occlusion may not fit together, especially if the upper and lower incisors erupt edge-to-edge. Because the patient may not be able to comfortably bite, they may accommodate by positioning their mandible forward resulting in an anterior cross bite. 2,3 But a far more common phenomenon that very few dentists understand is the problem resulting from a lower first molar erupting too far buccally. This also occurs at age 6. Then, typically at about age 6.5 the upper first molar erupts. The event of the upper first molar first coming into contact with the lower first molar is the most important day in any patient’s dental life! On this day, the mandible decides where to position itself. This often leads to asym-metric and/or aberrant positioning of the condyles in the fossa, asymmetric functioning of the facial and mastica-tory musculature, occlusal problems, speech impediments, periodontal complications, premature loss of lower first molars, improper development of the arch forms, canted occlusal planes, unacceptable prosthetic prognosis, etc. There may or may not be associated crossbite when a lower first molar erupts too far buccally. But the phenomenon often results in an aberrant position of the mandible and associated TMJ positions. In short, this is the most important principle of occlusion and virtually no dental professionals under-stand it. Certainly, zero dental school professors or occlusion gurus ever mention this. WhAT cAusEs AN AbERRANT JAW posiTioN? (AkA, A fuNcTioNAl shifT) Fig. 5 Fig. 6 WhEN A loWER fiRsT MolAR ERupTs Too fAR buccAlly, WE ofTEN sEE (fig. 4-6): ᕡ Facial asymmetry ᕢ A canted occlusal plane ᕣ Anterir and/or posterior open bite ᕤ Speech impediments (that no speech therapist has a fighting chance of correcting) ᕥ Compromised upper anterior tooth aesthetics ᕦ Parafunction and occusal wear ᕧ Myofacial pain ᕨ TMJ symptoms www.orthodontics.com Summer 2017 15
Journal of the American Orthodontic Society Summer 2017/Buyer's Guide: Page 15