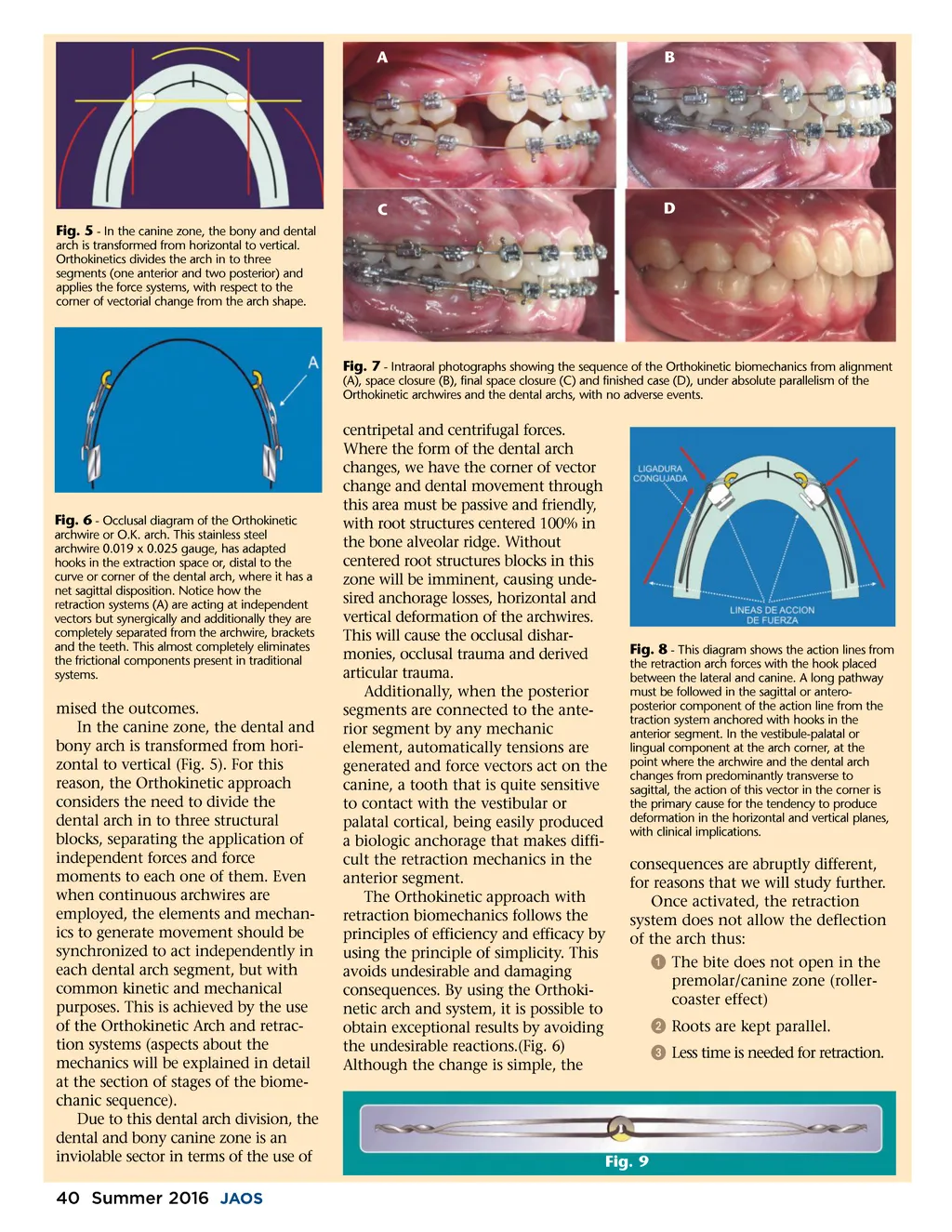
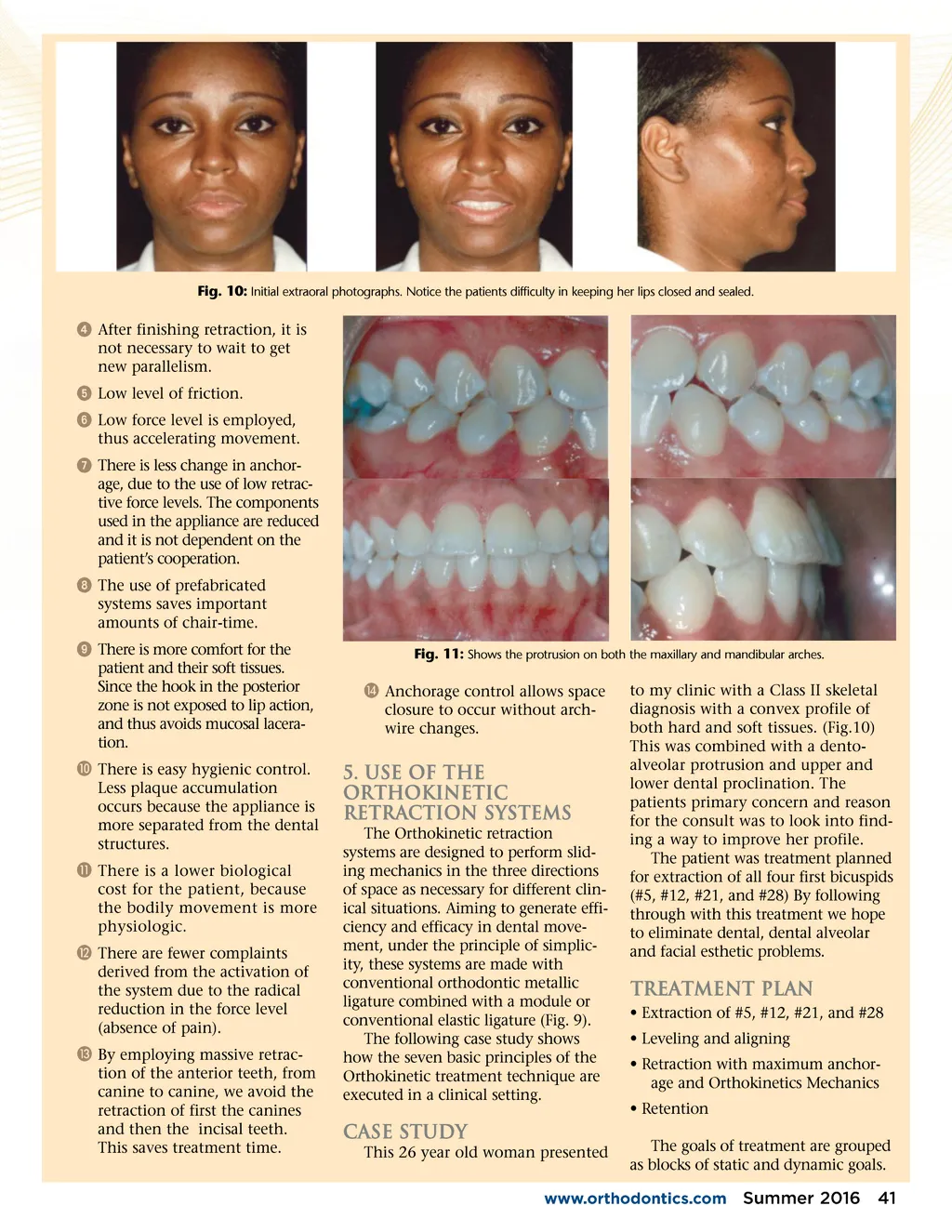
Fig. 10: Initial extraoral photographs. Notice the patients difficulty in keeping her lips closed and sealed. ᕤ After finishing retraction, it is not necessary to wait to get new parallelism. ᕥ Low level of friction. ᕦ Low force level is employed, thus accelerating movement. ᕧ There is less change in anchor-age, due to the use of low retrac-tive force levels. The components used in the appliance are reduced and it is not dependent on the patient’s cooperation. ᕨ The use of prefabricated systems saves important amounts of chair-time. ᕩ There is more comfort for the patient and their soft tissues. Since the hook in the posterior zone is not exposed to lip action, and thus avoids mucosal lacera-tion. µ There is easy hygienic control. Less plaque accumulation occurs because the appliance is more separated from the dental structures. ¸ There is a lower biological cost for the patient, because the bodily movement is more physiologic. ¹ There are fewer complaints derived from the activation of the system due to the radical reduction in the force level (absence of pain). Ƹ By employing massive retrac-tion of the anterior teeth, from canine to canine, we avoid the retraction of first the canines and then the incisal teeth. This saves treatment time. Fig. 11: Shows the protrusion on both the maxillary and mandibular arches. ƹ Anchorage control allows space closure to occur without arch-wire changes. 5. Use of the Orthokinetic Retraction Systems The Orthokinetic retraction systems are designed to perform slid-ing mechanics in the three directions of space as necessary for different clin-ical situations. Aiming to generate effi-ciency and efficacy in dental move-ment, under the principle of simplic-ity, these systems are made with conventional orthodontic metallic ligature combined with a module or conventional elastic ligature (Fig. 9). The following case study shows how the seven basic principles of the Orthokinetic treatment technique are executed in a clinical setting. to my clinic with a Class II skeletal diagnosis with a convex profile of both hard and soft tissues. (Fig.10) This was combined with a dento-alveolar protrusion and upper and lower dental proclination. The patients primary concern and reason for the consult was to look into find-ing a way to improve her profile. The patient was treatment planned for extraction of all four first bicuspids (#5, #12, #21, and #28) By following through with this treatment we hope to eliminate dental, dental alveolar and facial esthetic problems. Treatment Plan • Extraction of #5, #12, #21, and #28 • Leveling and aligning • Retraction with maximum anchor-age and Orthokinetics Mechanics • Retention The goals of treatment are grouped as blocks of static and dynamic goals. Case Study This 26 year old woman presented www.orthodontics.com Summer 2016 41
Journal of the American Orthodontic Society Summer 2016 / Buyer's Guide: Page 41