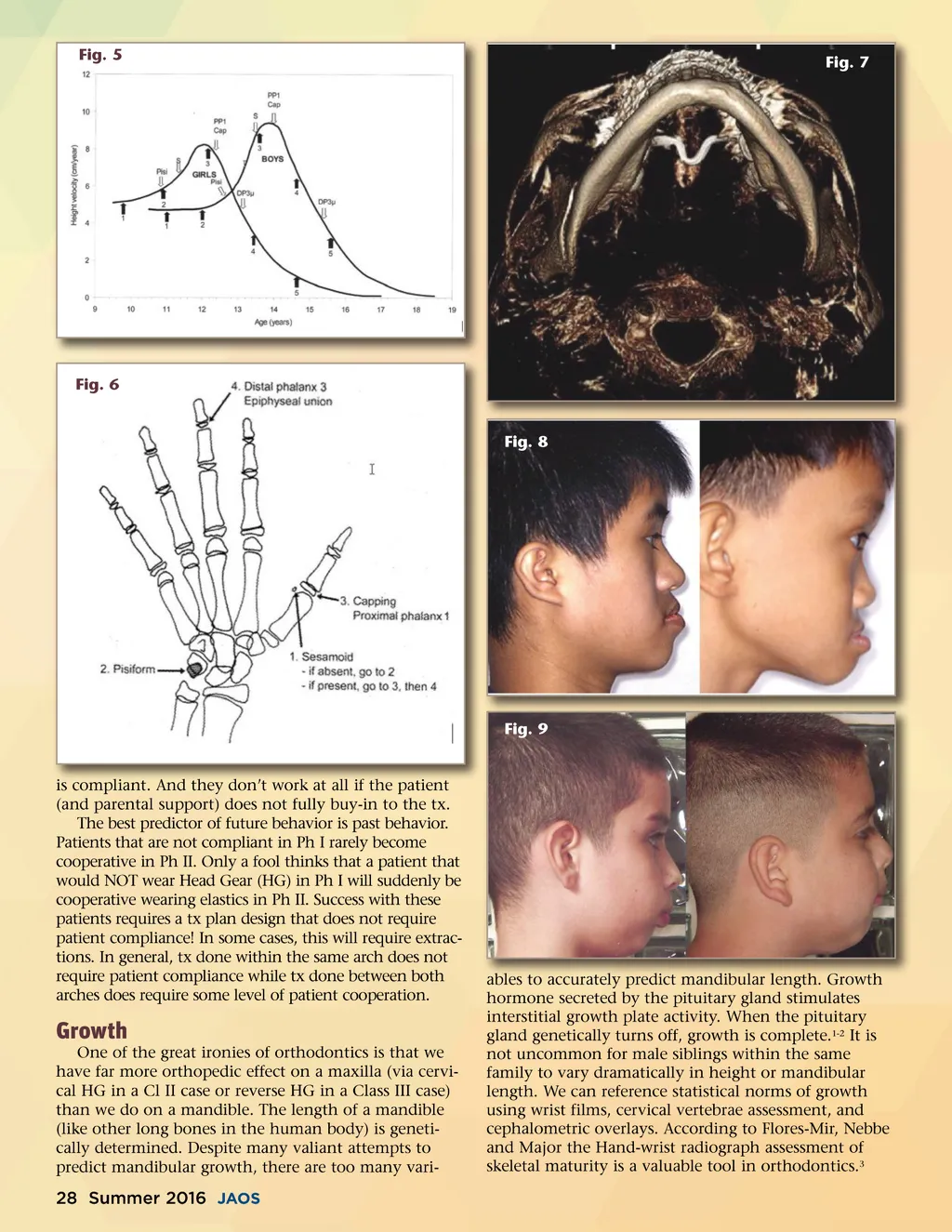
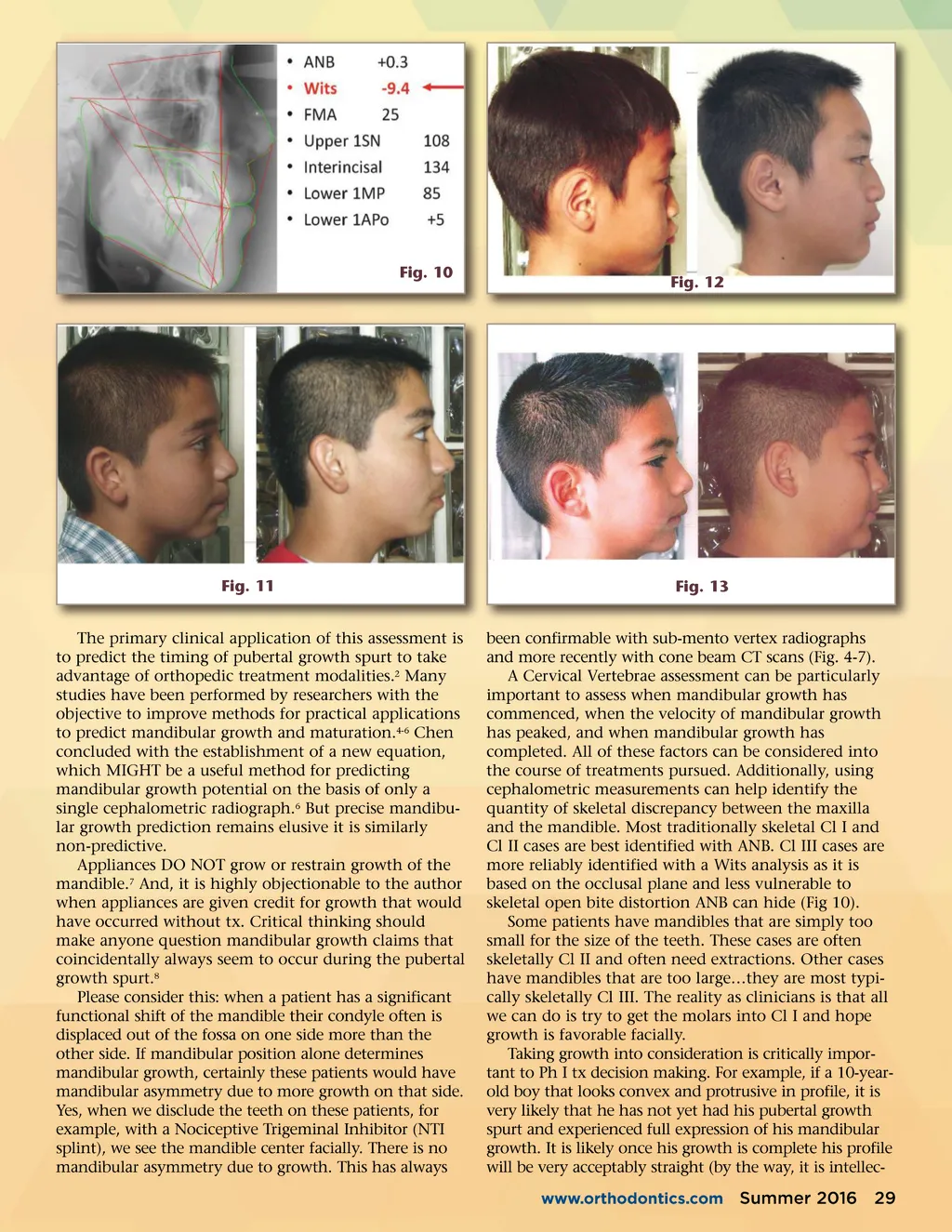
Fig. 10 Fig. 12 Fig. 11 The primary clinical application of this assessment is to predict the timing of pubertal growth spurt to take advantage of orthopedic treatment modalities. 2 Many studies have been performed by researchers with the objective to improve methods for practical applications to predict mandibular growth and maturation. 4-6 Chen concluded with the establishment of a new equation, which MIGHT be a useful method for predicting mandibular growth potential on the basis of only a single cephalometric radiograph. 6 But precise mandibu-lar growth prediction remains elusive it is similarly non-predictive. Appliances DO NOT grow or restrain growth of the mandible. 7 And, it is highly objectionable to the author when appliances are given credit for growth that would have occurred without tx. Critical thinking should make anyone question mandibular growth claims that coincidentally always seem to occur during the pubertal growth spurt. 8 Please consider this: when a patient has a significant functional shift of the mandible their condyle often is displaced out of the fossa on one side more than the other side. If mandibular position alone determines mandibular growth, certainly these patients would have mandibular asymmetry due to more growth on that side. Yes, when we disclude the teeth on these patients, for example, with a Nociceptive Trigeminal Inhibitor (NTI splint), we see the mandible center facially. There is no mandibular asymmetry due to growth. This has always Fig. 13 been confirmable with sub-mento vertex radiographs and more recently with cone beam CT scans (Fig. 4-7). A Cervical Vertebrae assessment can be particularly important to assess when mandibular growth has commenced, when the velocity of mandibular growth has peaked, and when mandibular growth has completed. All of these factors can be considered into the course of treatments pursued. Additionally, using cephalometric measurements can help identify the quantity of skeletal discrepancy between the maxilla and the mandible. Most traditionally skeletal Cl I and Cl II cases are best identified with ANB. Cl III cases are more reliably identified with a Wits analysis as it is based on the occlusal plane and less vulnerable to skeletal open bite distortion ANB can hide (Fig 10). Some patients have mandibles that are simply too small for the size of the teeth. These cases are often skeletally Cl II and often need extractions. Other cases have mandibles that are too large…they are most typi-cally skeletally Cl III. The reality as clinicians is that all we can do is try to get the molars into Cl I and hope growth is favorable facially. Taking growth into consideration is critically impor-tant to Ph I tx decision making. For example, if a 10-year-old boy that looks convex and protrusive in profile, it is very likely that he has not yet had his pubertal growth spurt and experienced full expression of his mandibular growth. It is likely once his growth is complete his profile will be very acceptably straight (by the way, it is intellec-www.orthodontics.com Summer 2016 29
Journal of the American Orthodontic Society Summer 2016 / Buyer's Guide: Page 29