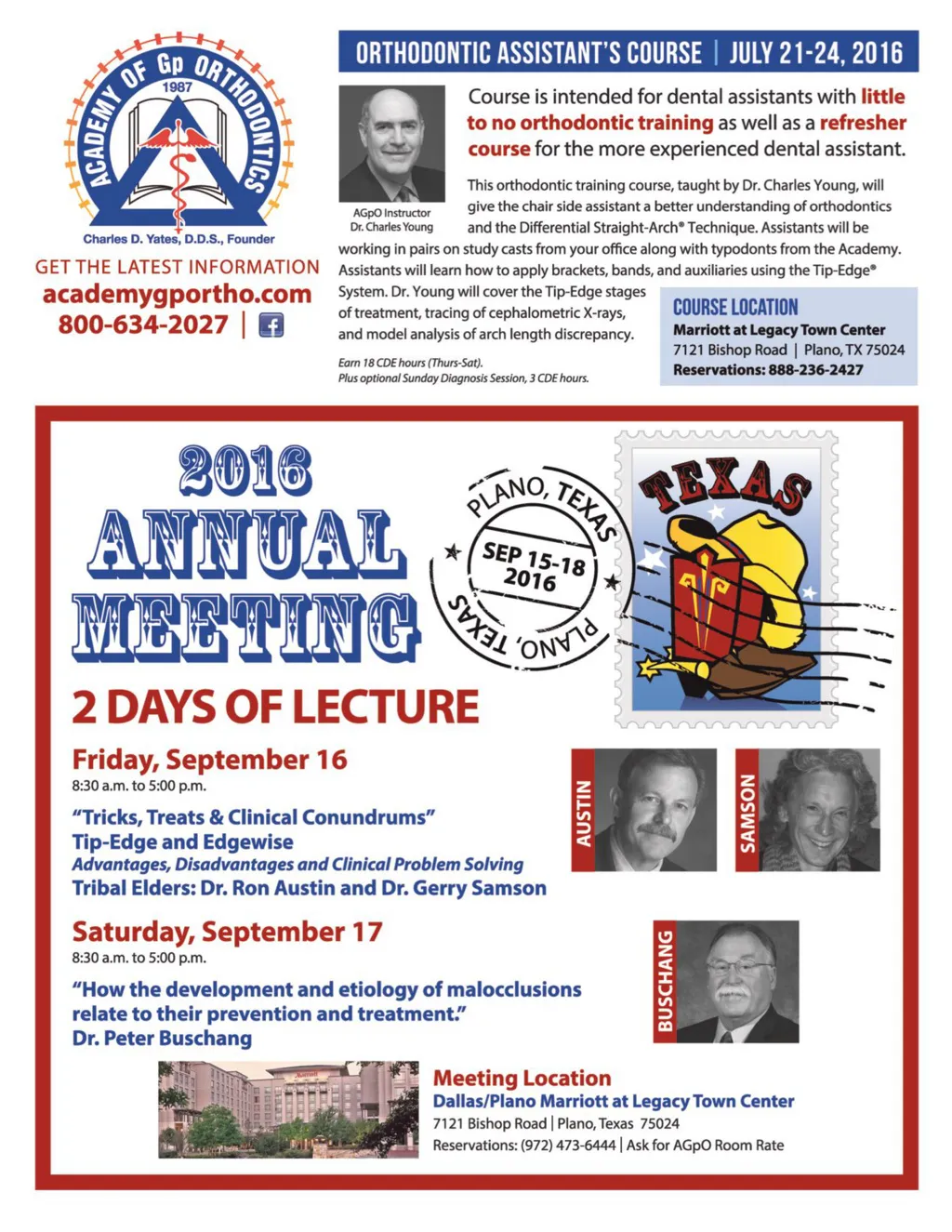
Fig. 14 Fig. 15 tually dishonest to ascribe this growth to any Ph I tx appliance when the growth is the true cause of the improved profile aesthetics) (Fig. 11-15). After all, don’t most adults appear to facially have ample mandibular length and chin? Just look around any crowded room. Growth unfortunately does not fix Cl II. If it did why do so many adults still have Cl II? This is something we must facilitate with our orthodontic treatment! Interestingly, the growth of the mandible is geneti-cally determined while the maxillary growth is deter-mined by the occlusal envi-ronment the erupted teeth have established. 9-11 One example would be in a Cl III case. If an anterior crossbite is not corrected before the pubertal growth spurt, there is nothing to restrain aggres-sive and excessive lower incisor advancement result-ing in severe dental/skeletal Cl III occlusal relationship. In some instances, rendering the case best treated with orthognathic surgery. But, on the other hand, if an anterior crossbite is corrected early in a child before the pubertal growth spurt there will be wonderful dental and skeletal outcomes! The coupled anterior overjet occlusion: (Fig. 16) A) Will restrain how far the lower incisors advance often resulting in very retroclined lower anterior teeth. B) Will stimulate the development of the premaxilla and “A” point resulting in far less skeletal Cl III. In general, two-phase orthodontic approach remains controversial. While some studies suggest that the same results can be achieved by single phase orthodontic treat-ments they do not take into consideration the benefits it has for the patient. 12 For example having an overbite or anterior crossbite can harvest years of ridicule and embarrassment while the patient is going through an important stage of self-identity. As a result low self-esteem can scar them for years. Furthermore a simple extraction case may develop into a complex surgical case if not treated by interceptive orthodontics. As mentioned earlier parents should never be insured that interceptive orthodontics is going to result in non-extraction tx. Also, “In general, two-phase orthodontic approach remains controversial. While some studies suggest that the same results can be achieved by single phase orthodontic treatments they do not take into consideration the benefits it has for the patient.” patients should never be quoted for a two-phase treat-ment as the outcome of Ph 1 is not guarantee. Here’s the rub: even though a patient’s mandible might profoundly grow during the pubertal growth spurt, the interdigitation of the posterior teeth most often does not permit growth to correct dental Cl II! So growth of the mandible and the dental classifica-tions are essentially inde-pendent events. Nonethe-less growth is critically important. In summary, there is also ample clinical evidence for clinicians that it is critically important they understand how growth has A-P implica-tions in both Cl II and Cl III cases: í In Cl II cases correction of the deep bite can facili-tate lower incisor advance-ment and some Cl II correction. í In Cl III cases creating some deep bite can create restraint on how much the lower incisors advance and dramatically reduce the amount of anterior crossbite remaining to correct. This can certainly reduce the need for lower extractions and often specialist recommended orthognathic surgery after full eruption. (see final diagram) In the third and fourth installments of this article, we will detail expanded explanations and examples of how to treat these conditions. How these problems are sequenced can largely depend on severity, priority, growth, and time till full eruption. Fig. 16 30 Summer 2016 JAOS
Journal of the American Orthodontic Society Summer 2016 / Buyer's Guide: Page 30